6주간의 고강도 간헐적 트레이닝이 20대 과체중 남성의 신체구성, 유산소 운동능력, 심혈관기능 및 혈액성분에 미치는 영향
Effects of 6 Weeks of High Intensity Intermittent Training on Body Composition, Aerobic Capacity, and Blood Variables in Overweight Males
Article information
Abstract
이 연구는 6주간 실시한 고강도 간헐적 트레이닝(high-intensity intermittent training: HIIT)과 중강도 지속적 트레이닝(moderate-intensity continuous training: MICT)이 20대 과체중 남성의 신체구성, 유산소 운동능력, 심혈관기능 및 혈액성분에 미치는 영향을 규명하는데 목적이 있다. 이 연구의 대상자는 체질량지수 25 kg·m-2 이상의 20대 과체중 남성 29명이었으며, 이들을 HIIT집단(n=11), MICT집단(n=10), 그리고 통제집단(n=8)에 무선 할당하였다. HIIT집단은 6주간 주 3회, 일일 25분 운동을 실시하였고, MICT집단은 동일한 기간 동안 주3회, 일일 33분 운동을 실시하였으며, 두 운동 간 에너지 소비량을 동일하게 하였다. 통제집단은 동일한 처치 기간 동안 특별한 처치 없이 평소의 생활 습관을 유지하도록 하였다. 처치 전·후에 신체구성, 유산소 운동능력, 심혈관기능, 인슐린 저항성, 그리고 혈중지질을 측정한 후 반복 이원변량분석을 이용하여 집단 간, 그리고 시기 간에 비교하였다. 이 연구의 주요 결과는 다음과 같다. 1) HIIT집단에서 체중, BMI, 체지방량, 그리고 허리-엉덩이둘레비가 유의하게 감소되었다. 2) VO2max, VEmax, 그리고 최대운동부하검사 시 탈진까지 소요된 시간에서 집단과 시기의 상호작용이 유의하게 나타났으며, HIIT 집단의 수치가 다른 두 집단에 비해 유의하게 높은 것으로 나타났다 3) HIIT집단에서만 수축기 혈압이 유의하게 감소되었으며, 안정시 심박수는 감소하는 경향이 나타났다. 4) 인슐린 저항성과 관련된 모든 변인에서 통계적으로 유의한 변화가 나타나지는 않았으나, 공복 인슐린과 HOMA-IR이 HIIT집단에서만 개선되는 경향을 보였다. 5) 혈중 지질과 관련된 모든 변인에서 통계적으로 유의한 변화가 나타나지 않았으나, HDL-C와 TG가 HIIT집단에서만 개선되는 경향을 보였다. 이상의 결과를 종합하면, 6주간의 HIIT 처치가 MICT에 비하여 유산소 운동능력과 심혈관기능의 향상에 더 긍정적인 영향을 미쳤으며, 신체구성, 인슐린 저항성 및 혈중 지질의 개선 가능성이 제시되었다.
Trans Abstract
The primary purpose of this study was to investigate the effects of 6 weeks of high-intensity intermittent training (HIIT) and moderate-intensity continuous training (MICT) under relatively equal energy expenditure on body composition, aerobic capacity, cardiovascular function, insulin resistance, and blood lipid profiles in 20s overweight males. Twenty-nine males were randomized into one of the following groups: HIIT group (n=11), MICT group (n=10), and control group(n=8). Subjects in HIIT group completed 6 weeks of training for 25 min/sessions, three times/wk, and subjects in MICT group exercised for 33 min/session to equalize the energy expenditure with HIIT group. Subjects in control group were asked to maintain their normal life pattern during the same intervention period. Data were analyzed using two-way repeated measures ANOVA with post hoc test. Main results of the present study were as follows: 1) Body weight, BMI, fat mass, and WHR decreased significantly in HIIT group. 2) VO2max, VEmax, and time to exhaustion increased significantly in HIT group. 3) SBP decreased significantly in HIIT group and HRrest was tended to decrease in HIIT. 4) Fasting plasma insulin and HOMA-IR were tended to decrease in HIIT, but the changes failed to reach the statistically significant level. 5) HDL-C and TG were tended to improve in HIIT, but the changes failed to reach the statistically significant level. Results indicate that high intensity intermittent exercise training is more beneficial in aerobic capacity and cardiovascular function. It was also suggested that 6 weeks of aerobic exercise training in either high intensity intermittent or moderate intensity continuous was not sufficient enough to induce changes in body composition, insulin resistance and blood lipid profiles.
서 론
비만을 해결하기 위한 대표적인 유산소 운동으로 조깅이나 걷기와 같은 중강도 지속적 운동(moderate-intensity continuous training: MICT)이 주로 사용되어 왔다(Boutcher, 2011; Jensen et al., 2014). 그 동안 비만의 개선에 더하여 혈압 감소(Cornelissen et al., 2013), 근질환 개선(Brum et al., 2014), 그리고 당뇨병 치료(Hansen et al., 2009) 등 MICT의 효과가 다양하게 검증되었으나, 일부 연구에서는 체중 조절에서는 상대적으로 적은 수준의 감량이 나타나 비만의 해소방법으로 효율적인 것인가 대한 문제가 제기되었다(Wu et al., 2009). 더욱이 장시간 운동이 지속되어야만 효과가 나타나는 부담감으로 인하여 중도 포기율이 높은 것으로 보고된 바 있고, 개인 생활과 학업 등으로 인하여 시간적 제약이 존재하는 사람들이 실천하기에는 어려운 운동방법으로 평가되고 있다. 실제로 보건복지부에서 운동을 하지 않는 사람들을 대상으로 그 이유를 조사한 결과, ‘시간 부족’이 가장 큰 이유인 것으로 조사되어(Ministry of Health and Welfare, 2013) 시간적 문제를 해결하고 비만자들의 운동 지속성을 향상시키기 위한 새로운 운동 프로그램이 요구되고 있다.
이에 최근 고강도 간헐적 트레이닝(high-intensity intermittent training: HIIT)에 대한 연구가 다수 보고되고 있다(ACSM, 2015). HIIT란 반복되는 짧은 시간의 고강도 운동과 저강도 운동 또는 휴식이 결합된 운동으로서(Trapp et al., 2008), 심혈관계 질병의 유병률과 인슐린 민감성 등과 같은 대사적 문제를 완화시키는데 효과적인 것으로 보고되어 MICT보다 더 효율적인 운동방법으로 조명 받고 있다(Boutcher, 2011; Heydari et al., 2012). 관련 선행연구에서, HIIT는 운동 중 카테콜라민의 증가를 통하여 피하지방의 지방 산화를 유도함으로써 체지방률을 감소시키고(Trapp et al., 2007; Boutcher, 2011), 운동 후에는 식욕을 감퇴시켜 음식 섭취를 낮추는 효과를 갖는다(Bilski et al., 2009). 또한 미토콘드리아 효소를 활성 시키고 지방 산화를 향상시키는 과정을 통하여 체중 감소에 영향을 미치는 것으로 보고되었다(Burgomaster et al., 2006). 이와 더불어 인슐린 저항성을 개선시켜 당뇨병과 관련된 대사 위험 요인을 개선하는데 큰 영향을 끼치며(Trapp et al., 2008), VO2peak를 증가시켜 심혈관계와 골격근 기능을 향상시키는데 효과적인 것으로 알려져 있다(Pattyn et al., 2014).
HIIT와 MICT의 효과를 비교하여 기술하면 다음과 같다. 과체중 남성에게 16개월간 주당 5시간 MICT를 처치한 결과 내장지방이 23% 감소된 것에 비하여(Donnelly et al., 2003), HIIT의 경우 3개월간 주3회, 회당 20분의 운동만으로도 내장지방이 17% 감소되었다(Heydari et al., 2012). Trapp et al.(2008)은 젊은 여성을 대상으로 15주간 회당 20분 HIIT를 실시한 집단과 회당 40분 MICT를 실시한 집단으로 분류하여 비교한 결과, MICT집단에서는 유의한 효과가 나타나지 않았으나, 상대적으로 적은 운동시간을 적용한 HIIT집단에서는 지방량의 유의한 감소가 나타났다. 이는 HIIT 운동법이 MICT와 비교하였을 때, 더욱 효과적이라는 것을 시사한다. 이와 더불어 Pattyn et al.(2014)은 관상동맥 환자들을 대상으로 MICT와 HIIT를 비교한 결과, 두 가지 운동 형태 모두에서 VO2max가 증가되었으나, HIIT집단에서 더 큰 폭의 증가가 나타났다고 보고하였다.
기간에 따른 HIIT의 효과와 관련된 논문을 살펴보면, Heydari et al.(2012)은 과체중 남성을 대상으로 20분간의 HIIT를 주3회의 빈도로 처치한 결과, 6주 후 시점에서 허리둘레가 유의하게 감소된 것으로 나타났다. 또한 Dunn et al.(2014)은 HIIT를 실시한지 6주 후 시점에서 공복 인슐린, HOMA-IR, 그리고 IL-6가 유의하게 감소되었다고 보고하였으며, 단 2주간의 HIIT 실시만으로도 최대산소섭취량, 인슐린 민감성, 그리고 허리둘레 등에 긍정적인 효과가 나타난 것으로 보고된 바 있다(Whyte et al., 2010). 더욱이 HIIT는 운동을 지속할 수 있는 수준이 상대적으로 높은 것으로 나타났다(Lau et al., 2015). 지나친 고강도 운동은 비만자들에게 부정적인 측면이 있을 수 있지만, HIIT가 과학적인 절차에 따라 그 효과가 검증된 것으로 보인다.
이상의 내용을 종합해 보면, 선진 외국을 중심으로 HIIT의 효과를 검증하는 연구가 다수 수행되어 왔고, HIIT의 효과를 MICT와 비교하는 연구도 일부 이루어져 왔다. 그러나 국내에서는 HIIT의 효과를 검증한 연구가 매우 제한적이어서 이에 대한 연구가 필요하다. 그리고 HIIT와 MICT의 효과를 비교하는 과정에서 두 가지 다른 형태의 운동의 양을 동질화시키지 못하여 비교를 하는데 한계가 있었다. 따라서 두 가지 운동의 양을 같게 하여 보다 정확하게 비교하는 연구가 필요하다. 이 연구는 이와 같은 필요성을 충족하고자 시도되었으며, 특히 한 연구에서 HIIT와 MICT가 다양한 종속변인에 미치는 영향을 동시에 비교하였다는 점에서도 의미가 있다고 사료된다. 아울러 트레이닝의 지속율이 떨어지는 비만자를 대상으로 하여 상대적으로 짧은 기간에 운동의 효과가 나타나는 것으로 알려진 HIIT의 단기간 실시가 실제로 효과가 있다면 비만자를 위한 효과적인 운동이 될 수 있을 것임에도 불구하고, 비만자를 대상으로 단기간의 HIIT 수행을 통하여 신체 기능의 개선이 이루어지는지에 대한 연구가 매우 부족하여 이 연구를 수행하게 되었다. 본 연구에서는 6주간 HIIT와 MICT의 처치가 20대 과체중 남성의 신체구성, 유산소 운동능력, 심혈관기능, 인슐린 저항성 및 혈중 지질에 미치는 영향을 규명하고자 하였다.
연구방법
연구 대상자
이 연구의 대상자는 G도 소재의 K대학교에 재학 중인 20대 남성으로서 체질량지수가 25 kg·m-2 이상인 자, 최근 6개월간 체계적인 트레이닝에 참여한 경험이 없는 자, 그리고 심혈관계 및 근골격계 질환이 없으며 대사적 질병으로 인하여 복용하는 약이 없는 자로 제한하였다. 연구 참여 기준에 따라 29명의 대상자를 선정하여, 1) HIIT집단 11명, 2) MICT집단 10명, 그리고 3) 통제집단에 8명으로 무선 할당(random assignment)하였다. 실험에 앞서 본 연구의 내용과 절차에 대해 충분히 설명하였고, 자발적으로 참가하고자 하는 자로부터 검사동의서를 받은 후 연구에 참여하도록 하였다. 이 연구의 대상자의 신체적 특성은 <Table 1>에 제시된 바와 같다.

Characteristics of subjects
(Mean±SD)
연구 설계와 절차
이 연구의 독립변인은 HIIT와 MICT이었으며, 주요 종속변인은 신체구성, 유산소 운동능력, 심혈관기능, 인슐린 저항성 지표, 그리고 혈중 지질이었다. 6주간의 처치에 따른 변화를 비교하였다. 이 연구의 절차를 도식화하여 제시하면 <Figure 1>과 같다.
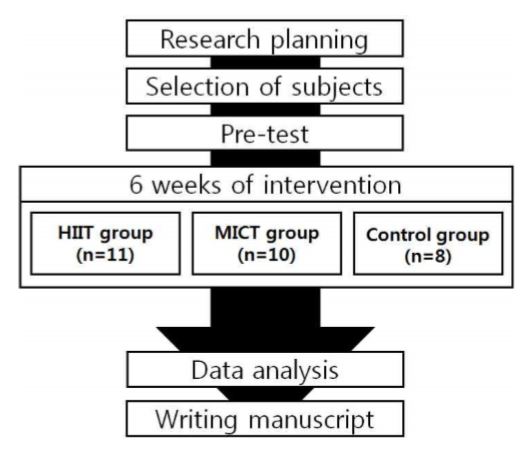
Procedure of study
측정 항목과 방법
1) 체격과 신체구성
신장의 측정은 수동식 일반 신장계(삼화, 한국)를 이용하여 측정하였으며, 체중은 전자식 저울(CAS-150, 한국)을 이용하여 측정하였다. 신체구성은 체성분 분석기(자원메디칼, 한국)를 이용하여 체지방률(%), 체지방량(㎏), 그리고 제지방량(㎏)을 측정하였으며, BMI는 체중을 신장의 제곱으로 나누어 계산하였다. 허리둘레는 갈비뼈의 맨 아래와 장골능 사이의 중간 부위에서 측정 하였고, 엉덩이둘레는 엉덩이의 최대돌출부위에서 측정하였으며, 허리둘레를 엉덩이둘레로 나누어 허리-엉덩이둘레비(waist hip ratio: WHR)를 산출하였다.
2) 유산소 운동능력
최대산소섭취량(VO2max)을 분석하기 위하여 가스분석기(Ultima CPX, Med Graphics, 미국)와 트레드밀(STEX8100TD, 한국)을 사용하여 최대운동부하검사를 실시하였다. 검사방법으로 Bruce protocol을 적용하였다. 대상자가 운동을 더 이상 지속할 수 없을 때까지 실시하였으며, 운동 중지 후 5분간 정리운동을 실시하였다(Bruce et al., 1973). 가스분석을 통해 20초 간격으로 VE, VCO2, 그리고 VO2를 관찰하였으며, 최대운동부하검사 동안 VO2가 가장 높았던 3가지 시점의 평균을 VO2max로 기록하였다.
3) 심혈관기능
대상자가 12시간 이상 공복을 유지한 상태로 실험 당일 오전 8시에 검사실에 도착하여 30분간 안정을 취하도록 한 후 혈압과 심박수를 측정하였다. 혈압의 경우 수은혈압계를 이용하여 수축기 혈압(systolic blood pressure: SBP)과 이완기 혈압(diastolic blood pressure: DBP)을 측정하였고, 심박수는 1분간 촉진법(palpation)을 이용하여 측정하였다.
4) 혈액 채취 및 성분 분석
혈압과 심박수를 측정한 직후 1회용 주사기로 상완주정맥에서 혈액을 채취한 뒤, 3000 rpm으로 10분간 원심 분리하여 (주)G의료재단에 분석을 의뢰하였다. 인슐린 저항성 변인으로 글루코스, 인슐린, 그리고 HbA1c을 검사하였으며, HOMA-IR(homeostasis model for insulin resistance)은 아래의 Matthews et al.(1985)의 공식을 이용하여 산출하였다.
▸HOMA-IR=[글루코스(mmol·ℓ-1)×인슐린(μU·㎖-1)]/22.5
혈중 지질의 변인으로는 TC, TG, HDL-C 및 LDL-C를 검사하였으며, LDL-C는 TG 수치가 400 mg·㎗-1이하일 경우, Friedewald et al.(1972)이 제안한 아래의 추정공식을 이용하여 산출하였다.
▸LDL-C=TC(mg·㎗-1)-[HDL-C(mg·㎗-1)+TG(mg·㎗-1)/5]
트레이닝 프로그램
본 연구에서 트레이닝을 실시한 두 집단의 대상자는 트레드밀(Precor C956i, 미국)에서 각각 다른 형태로 달리기를 실시하였다. 두 집단에서 실시한 운동 간에 운동 강도와 시간의 차이가 있었지만 1회 운동 중 소비되는 산소소비량을 동일하게 하였다.
두 집단의 총 운동양은 Rognmo et al.(2004)이 제시한 방법에 따라 동질화 시켰다. 이 연구 대상자의 사전 평균 VO2max는 3.63 ℓ·min-1이었다. HIIT 처치 시 3.27 ℓ·min-1(VO2max의 90%)수준에서 4분 × 4회 운동을 하였을 때의 산소소비량과 2.18 ℓ·min-1(VO2max의 60%) 수준에서의 3분 × 3회 운동하였을 때의 산소소비량의 총합은 71.87 ℓ·min-1이었다. 따라서 HIIT 운동 중 총 산소소비량을 MICT의 강도의 산소소비량으로 나누어(71.87/2.18 ℓ·min-1) 총 33분의 본운동 시간을 산출하였다. 두 집단의 트레이닝 프로그램을 자세히 살펴보면 다음과 같다.
1) HIIT집단
준비운동과 정리운동은 VO2max의 50∼60% 강도로 각각 5분과 3분간 실시하였다. 준비운동을 마친 후 VO2max의 80∼90% 강도로 4분간의 운동을 수행하였으며, 이를 4회 반복하였다. 고강도 운동 사이에는 VO2max의 50∼60% 강도의 중강도 운동을 3분간 실시하게 하여 인터벌 운동의 특성을 유지하도록 하였다. 즉, 본운동 시간은 25분이었으며, 주3회의 빈도로 총 6주간 실시하였다. 운동 프로그램 내 설정된 운동시간을 대상자에 정확히 알리기 위하여 운동이 종료되기 전 시점을 구두로 카운트 하였으며, 이를 통해 대상자가 의식적으로 속도를 조절할 수 있도록 보조하였다.
2) MICT집단
준비운동과 정리운동은 VO2max의 50∼60% 강도로 각각 5분과 3분간 실시하였다. 준비운동을 마친 후 VO2max의 50∼60% 강도로 33분간의 본운동을 수행하였으며, 주3회의 빈도로 총 6주간 실시하였다.
3) 통제집단
6주의 동일한 처치 기간 동안 통제집단 대상자는 평소의 신체활동과 식이습관을 유지하도록 하였다.
이상에서 기술한 세 집단에 있는 모든 대상자들이 6주의 처치 기간 동안 매주 1회 이상 연락하여 평소의 식이습관을 그대로 유지하도록 하였다.
자료처리 방법
본 연구에서 얻은 모든 자료는 SPSS PC+ for Windows(version 22.0) 통계 프로그램을 이용하여 분석하였다. 각 집단에서 얻은 각 종속변인의 기술 통계량을 평균(mean)과 표준편차(standard deviation: SD)로 제시하였다. 세 집단(HIIT집단, MICT집단, 그리고 통제집단) 간, 그리고 두 시기(사전검사 시기, 사후검사 시기) 간 종속변인의 평균 차이를 검증하기 위하여 반복 이원변량분석(two-way ANOVA with repeated measures)을 실시하였다. 집단의 주효과, 시기의 주효과, 또는 집단과 시기의 상호작용이 유의한 경우, 각 집단 내 두 시기 간 차이는 종속 t-검증(paired t-test)으로, 그리고 각 시기 내 세 집단 간의 평균의 차이는 일원변량분석(one-way ANOVA)과 최소유의차 검증법(least significant difference: LSD)을 실시하여 분석하였다. 모든 통계분석의 유의수준(α)을 .05로 설정하였다. 한편, G power, 3.1을 이용하여 유의수준 .05, 검정력 85%, 효과크기를 높은 수준인 0.35로 적용하여 총 대상자의 수를 산출하였다.
연구 결과
신체구성
HIIT집단의 경우 체중, BMI, 체지방량, 그리고 허리-엉덩이둘레비에서 유의한(p<.05) 감소가 나타났으며, MICT집단의 경우 체중(p<.05), BMI(p<.05), 그리고 허리-엉덩이둘레비(p<.01)에서 유의한 감소가 나타났다. 통제집단에서는 허리둘레와 엉덩이둘레에서 유의한(p<.01) 증가가 나타났다(Table 2).

Changes in body composition from pre- to post-training
(Mean±SD)
유산소 운동능력
VO2max, 최대운동부하검사 시 탈진까지 소요 시간, 그리고 VEmax에서 집단과 시기의 상호작용이 유의하게 나타났으며, 세 변인 모두 HIIT집단이 MICT집단과 통제집단에 비하여 유의하게 높게 나타났다. 또한 최대운동부하검사 시 탈진까지 소요된 시간에서 HIIT집단만 시기 간에 유의한(p<.01) 증가가 나타났다(Table 3).

Changes in aerobic capacity from pre- to post-training
(Mean±SD)
심혈관기능
심혈관기능과 관련된 모든 변인에서 집단과 시기의 상호작용이 유의하게 나타나지 않았으나, 수축기 혈압에서 시기의 주효과가 나타났다. 수축기 혈압의 경우 HIIT집단에서만 유의하게(p<.05) 감소된 것으로 나타났다. 안정시 심박수의 경우 HIIT집단에서 감소되는 경향이 나타났으며(8.27% 감소), 집단과 시기의 상호작용이 유의한 수준에 가까워(p=.061) 심혈관기능이 개선되는 경향을 보였다(Table 4).

Changes in cardiovascular function from pre- to post-training
(Mean±SD)
인슐린 저항성 지표
인슐린 저항성과 관련된 모든 변인에서 집단과 시기의 상호작용이 유의하게 나타나지 않았으나, HbA1c에서 시기의 주효과가 나타났다. 공복 인슐린은 HIIT집단에서 -33.74% 감소하여 집단과 시기의 상호작용이 유의한 수준에 가깝게(p=.053) 나타났다. HOMA-IR 역시 HIIT집단에서 -33.27% 감소하였고, 집단과 시기의 상호작용이 유의한 수준에 가까워(p=.072) 인슐린 저항성이 개선되는 경향을 보였다(Table 5).

Changes in insulin resistance from pre- to post-training
(Mean±SD)

논 의
신체구성의 변화
HIIT와 신체구성의 관계와 관련하여, 과체중 중년 남성을 대상으로 한 Tjønna et al.(2013)의 연구와 과체중 젊은 남성을 대상으로 한 Heydari et al.(2012)의 연구에서 HIIT를 실시한 결과 체중, BMI, 체지방률, 그리고 체지방량이 유의하게 감소된 것으로 나타났다. 또한 Yang & Choi(2011)는 비만 중년 여성을 대상으로 16주간 주5회 HIIT와 MICT를 실시한 결과 두 집단 모두 체지방률의 유의한 감소가 나타났으며, HIIT에서 더 큰 효과가 나타났다고 보고하였다. 더욱이 Hottenrott et al.(2012)은 내장지방을 감소하는데 있어 HIIT가 MICT보다 더 효과적이라고 주장하였으며, Slentz et al.(2009)은 운동 강도가 높을수록 지방의 감소율이 높아진다고 보고하였다. 이상의 선행 연구를 종합해보면, HIIT가 체중, BMI, 체지방률, 그리고 체지방량의 감소에 효과적이며, MICT에 비하여 더 큰 효과를 나타낸다는 사실을 알 수 있다. HIIT가 지방 감소에 더 효과적인 이유는 다음 선행논문들을 토대로 해석할 수 있다. Tjønna et al.(2008)은 HIIT가 지방산이 지방조직으로 이동하는 것을 감소시키는데 효과적이며, 지방 조직 안에서의 지방 합성을 감소시켜 전체적인 지방 대사를 개선시킨다고 보고하였다. 또한 운동 시 에너지원으로서 글리코겐의 사용을 줄이기 때문에 지방 산화를 증가시키는데 더욱 효과적인 운동법으로 보고된 바 있다(Heydari et al., 2012).
이 연구에서는 6주간의 처치 후 HIIT집단과 MICT집단 모두 근육량에서 통계적으로 유의한 변화가 나타나지 않았다. 이는 12주간 HIIT와 MICT를 실시하였을 때 근육량과 골밀도 등과 같은 골격근의 건강 요인들의 변화가 나타나지 않았다는 Nybo et al.(2010)의 연구 결과와 유사하다. 이 연구에서 체중과 체지방량의 유의한 감소가 있었음에도 불구하고, 사전과 비교하여 동일한 체내 근육량의 비율 유지에 효과가 있는 것으로 결론지을 수 있다. 또한 허리둘레와 엉덩이둘레에 대한 결과에서 집단과 시기의 상호작용이 유의하게 나타났으며, 허리-엉덩이둘레비의 경우 시기의 주효과가 유의하게 나타났다. 이와 관련한 선행연구로, Heydari et al.(2012)은 12주간 주3회 과체중의 젊은 남성을 대상으로 HIIT를 수행한 결과 허리둘레의 유의한 감소가 나타났다고 보고하였으며, Jung et al.(2011)은 대사증후군 환자를 대상으로 12주간 주5회 HIIT와 MICT를 처치한 결과 두 집단 간에 유의한 차이는 나타나지 않았으나 사전에 비하여 허리둘레의 유의한 감소가 나타났다고 보고하였다. 선행연구와 이 연구의 결과를 종합해보면 운동 시간이 더 짧은 HIIT가 MICT보다 허리둘레를 감소시키는데 더 효율적이었다고 판단된다. 한편, 통제집단에서 허리둘레와 엉덩이둘레가 유의하게 증가된 것은 6주의 처치 기간 동안 신체활동을 의도적으로 통제하여 실험 참여 전보다 운동을 더 하지 않은 것과 식이 통제가 완벽하게 이루어지지 못한 점 등으로 해석할 수 있다.
이상에서 전술한 내용을 종합해 보면, 20대 과체중 남자에게 6주간의 짧은 처치에도 불구하고 HIIT집단과 MICT집단 모두 비만 지표 개선에 효과적인 것으로 나타났다. 특히, HIIT가 MICT에 비하여 체지방률, 체지방량, 그리고 체중 감소에 더욱 효과적인 것으로 판단된다. 뿐만 아니라 허리둘레와 허리-엉덩이둘레비를 개선하는데 효율적인 것으로 사료되며, 더 나아가 복부 비만을 감소시켜 고혈압, 제2형 당뇨병, 고지혈증, 관상동맥질환, 그리고 조기 사망 위험률을 예방하는데 도움이 될 것이라고 판단된다.
유산소 운동능력의 변화
이 연구의 결과, VO2max의 경우 집단과 시기의 상호작용이 유의하게 나타났으며, 다른 두 집단에 비해 HIIT집단에서 유의하게 높은 수준이 나타났다. 이와 같은 결과를 지지하는 연구로, Tjønna et al.(2013)은 과체중 중년 남성을 대상으로 10주간 주3회 HIIT을 실시한 결과 VO2max가 13% 증가되었다고 보고하였으며, Helgerud et al.(2007)은 젊은 남성을 대상으로 8주간 주3회 운동을 실시한 결과 HIIT집단이 MICT집단에 비해 VO2max가 더 유의하게 증가되었다고 보고하였다. 이와 더불어 Milanovic et al.(2015)의 메타분석에서는 젊은 층에서 중년층까지 통제집단과 비교하였을 때 HIIT와 MICT집단 모두 VO2max의 향상이 나타났으며, HIIT집단이 MICT집단에 비해 더 큰 효과를 보였다고 보고하였다. 선행 연구들의 결과를 종합해 보면, HIIT는 MICT에 비하여 VO2max를 증가시키는데 더 큰 효과를 나타낸다는 사실을 알 수 있으며, 이는 이 연구의 결과가 일치한다.
최대운동부하검사 시 탈진까지 소요된 운동 시간을 살펴보면, 이 연구의 HIIT집단에서만 유의한 향상이 나타났다. 이와 같은 결과를 뒷받침하는 선행연구는 다음과 같다. Gleser & Vogel(1971)은 유산소 운동이 탈진까지의 운동 시간을 증가시켰으며, 이는 유산소 운동능력의 향상을 의미한다고 보고하였다. 이와 더불어 Hickson et al.(1977)은 고강도 유산소 운동이 운동 시간을 유의하게 증가시켰다고 언급하였다. 최대운동부하시간이 1분 감소할 때 고혈압의 위험이 19% 증가한다고 주장한 Cooney et al.(2010)의 연구와 본 연구 결과를 종합해보면, HIIT가 유산소 운동능력을 향상시키고 고혈압의 위험을 낮추며 이는 MICT보다 더 효과적인 것을 알 수 있다.
최대환기량(VEmax)과 관련된 선행논문을 살펴보면, Rognmo et al.(2004)은 관상동맥질환을 가지고 있는 환자를 대상으로 10주간 주3회 HIIT와 MICT의 처치를 실시하였을 때, 두 집단 모두 VEpeak가 증가되었으며 HIIT집단에서 더 큰 효과가 나타났다고 보고하였다. 또한 Helgerud et al.(2007)은 성인 남성을 대상으로 8주간 주3회 HIIT를 실시한 결과 VEmax가 통계적으로 유의하지는 않았지만 9.36% 향상되었다고 보고하였다. 이 연구에서는 VEmax의 경우 세 집단 모두에서 집단과 시기의 상호작용이 유의하게 나타났으며, HIIT집단이 MICT집단과 통제집단에 비하여 유의하게 높게 나타나 선행연구와 유사한 결과를 도출하였다. 이와 같이 HIIT 후 나타난 VEmax의 증가는 호흡근의 발달과 최대운동 시의 1회 환기량 및 호흡수의 증가에 기인한 것으로 사료된다(Wilmore & Costill, 2006). HIIT가 MICT보다 유산소 운동능력을 향상시키는 이유는 HIIT가 미토콘드리아를 활성화 시키는 PGC-1α 증가에 더욱 효과적이며, 근육 섬유와 근형질세망 사이의 Ca++흡수율을 증가시켜 미토콘드리아 능력을 향상시키고 좌심실의 1회 박출량을 증가시키기 때문으로(Wisløff et al., 2007; Tjønna et al., 2008) 사료된다.
이상에서 전술한 내용을 종합해 보면, 단기간의 MICT는 유산소 운동능력 향상에 영향을 주지 못한 반면, HIIT는 유산소 운동능력 향상에 효과적인 것으로 판단된다. 향후 유산소 운동능력 수준이 낮은 사람들을 대상으로 HIIT 처치의 기간을 늘려 장기간의 처치가 수행된다면 유산소 운동능력의 더욱 뚜렷한 변화를 기대할 수 있을 것으로 판단된다.
심혈관기능의 변화
유산소 운동을 실시함으로써 혈압과 심박수를 낮추어 심혈관 기능을 향상시킨다는 사실은 많은 연구를 통하여 입증되었으며(Spina, 1999), 최근 HIIT 운동법이 심혈관계 위험요인을 감소시키는데 현실적이고 효율적인 운동으로 소개되고 있다(Gibala et al., 2012). 이 연구에서 수축기 혈압의 경우, HIIT집단에서만 통계적으로 유의한 감소가 나타났으며(-5.05%), MICT집단에서는 유의한 감소는 나타나지 않았으나 사전에 비해 감소되는 경향이 나타났다(-4.65%). 이는 HIIT가 MICT에 비해 수축기 혈압 감소에 더욱 효과적이라고 보고한 선행연구(Nemoto et al., 2007)와 일치하는 내용이며, 성인 남성을 대상으로 12주간 주3회 HIIT와 MICT를 처치한 결과 HIIT가 심폐체력과 수축기 혈압을 개선시키는데 MICT보다 더 효과적이라고 보고한 Nybo et al.(2010)의 연구 결과와도 유사하였다.
HIIT가 MICT보다 혈압 감소에 더 효과적이라는 결과는 다음과 같은 선행 연구에 근거하여 해석될 수 있다. 첫째, 동맥의 경직은 고혈압 발생의 주원인으로서(Mitchell, 2014), 운동 후 동맥경직도의 감소는 혈압의 감소와 연결되며, MICT집단보다 HIIT집단에서 더 높은 동맥 경직도의 감소가 나타나 혈압 감소에 더 큰 영향을 끼친 것으로 나타났다(Ciolac, 2012). 둘째, 운동을 통한 내피세포 기능 향상은 혈압을 감소시키는데 효과적이며(Baster-Brooks & Baster, 2005), HIIT가 MICT에 비해 내피세포 기능 향상에 더 효과적이라고 보고되었다(Wisløff et al., 2007; Molmen-Hansen et al., 2012). Baster-Brooks & Baster(2005)는 수축기 혈압과 이완기 혈압의 2 mmHg 감소는 뇌졸중 위험을 각각 14%, 17% 감소시키며, 관상동맥질환을 각각 9%, 6% 감소시킨다고 보고하였다. 따라서 앞서 언급한 운동 처치 후 신경기능의 향상과 본 연구의 결과를 종합하면 HIIT가 MICT에 비해 수축기 혈압을 낮추는데 더 효과적인 것이며 나아가 심혈관계 질환을 예방하고 개선하는데 영향을 줄 것으로 사료된다.
본 연구에서 안정시 심박수의 경우 통계적으로 유의한 변화가 나타나지는 않았으나 HIIT집단에서 8.27% 감소되어 개선되는 경향을 보였다. Hottenrott et al.(2012)은 12주간 가벼운 활동을 하는 40대 남녀를 대상으로 HIIT를 실시한 결과 안정시 심박수의 유의한 감소가 나타났다고 보고하였으며, 이는 본 연구의 결과를 뒷받침 해주는 것으로 사료된다. Collier et al.(2009)은 운동 후 안정시 심박수가 감소하는 이유가 미주신경의 톤이 증가하고 교감신경이 감소함에 나타나는 것이라고 하였으며, 좌심실의 기능 향상으로 인한 1회 박출량의 증가가 심장의 스트레스 감소에 도움을 주기 때문이라고 설명하였다(Helgerud et al., 2007). 그러나 Gormley et al.(2008)은 6주간 20대 성인 남녀를 대상으로 어떠한 운동 강도에서도 안정시 심박수의 감소가 나타나지 않았다고 보고하였으며, Nybo et al.(2010)은 12주간 주3회 성인 남성을 대상으로 HIIT와 MICT를 처치하였을 때 MICT에서만 안정시 심박수의 유의한 감소가 나타났다고 보고하였다. 이와 같이 유산소 운동과 안정시 심박수의 관계를 규명하는 여러 선행연구에서 서로 상반된 결과가 보고되었다. 따라서 HIIT에 따른 안정시 심박수의 변화를 규명하기 위한 연구가 추가적으로 진행되어야 할 것으로 사료된다.
이상에서 기술한 내용을 종합해 보면, HIIT와 MICT는 20대 과체중 남성의 수축기 혈압을 감소시키는데 효과적이며 HIIT가 MICT 보다 수축기 혈압을 감소시키는데 효과적이다. 또한 HIIT는 안정시 심박수를 낮추어 심혈관계 질환을 예방하는데 잠재적인 효과가 있다고 사료된다. 추후 연구에서는 50대 이상의 사람은 이완기 혈압보다 수축기 혈압을 감소시키는 것이 심혈관계 위험요인을 낮추는데 더 중요하다고 제시한 NHBPEP(2004)의 보고서를 참고하여 혈압이 높은 50대 이상의 환자들을 대상으로 HIIT를 수행하였을 때 심혈관계 기능의 향상을 기대할 수도 있을 것이다.
인슐린 저항성 지표의 변화
불균형적인 피하지방과 복부지방의 축적으로 인하여 인슐린 수용기의 감각이 둔화되어 골격근 내로 글루코스의 흡수가 저하되면서 체내 글루코스 처리 기능에 장애를 초래하여 인슐린 저항성이 유발된다(Li et al., 2014). 높은 인슐린 저항성은 심혈관계 질환의 위험요인이며, 대사증후군과 제2형 당뇨병, 그리고 이상지질혈증 등의 질환 발병을 높인다(Meshkani & Adeli, 2009). 이와 더불어 2~3개월 동안의 혈당 조절을 반영하는 지표인 당화혈색소(HbA1c)의 수치가 높아질수록 대사증후군 발병위험이 증가하기 때문에 이를 낮추는 것이 중요하다(ACSM, 2013).
이 연구의 결과, 공복 인슐린과 HOMA-IR이 사전검사와 사후검사 간에 통계적으로 유의하게 변화되지는 않았지만 HIIT집단에서 인슐린(-33.74%)과 HOMA-IR(-33.27%)이 감소되는 경향을 보였으며, 세 집단 중 가장 뚜렷한 감소가 나타났다. 유사한 연구결과로, Jelleyman et al.(2015)의 메타분석에서 HIIT가 MICT에 비하여 인슐린 저항성 개선에 효과적이며, 그 효과는 대사증후군이나 제2형 당뇨병을 가진 사람들에게 더 크게 나타난다고 제시하였다. 또한 2주 동안 신체활동량이 낮은 성인을 대상으로 HIIT를 실시한 결과 인슐린 민감성은 증가되었으나 공복혈당은 변화가 없는 것으로 보고되었다(Richards et al., 2010). 또한 본 연구의 HIIT집단에서 인슐린이 감소하였음에도 불구하고 공복혈당의 변화가 없었던 점을 감안할 때, HIIT 처치가 인슐린 민감도를 향상시킬 가능성이 큰 것으로 보인다. HIIT가 MICT 보다 더 효과적인 이유를 생리학적으로 살펴보면, 간에서 글루코스 대사를 조절하는 아드레날린의 민감성 향상과(Vincent et al., 2004), GLUT4의 향상에 영향을 미치기 때문이다(Gibala et al., 2006). 따라서 HIIT 운동법은 대사증후군이나 제2형 당뇨병과 같은 대사 문제를 보유한 사람들에게 더욱 효과적인 운동법이 된다는 사실을 알 수 있다. 이 연구에서 관찰한 변인 중 당화혈색소(HbA1c)와 관련된 선행연구를 살펴보면, Jelleyman et al.(2015)의 메타분석에서, 대사증후군 환자와 제2형 당뇨병 환자가 HIIT를 실시한 경우, 통제집단에 비해 HbA1c가 유의하게 변화되었으나, 그 변화 폭이 MICT의 변화량과는 유의한 차이가 나타나지 않았다. 또한 Kang(2013)은 내당능장애 중년 여성을 대상으로 12주간 주5회 HIIT와 MICT를 실시하였을 때 두 처치 모두 HbA1c의 유의한 향상이 나타났으나, 두 집단 간의 차이는 없다고 하였다. 이 연구에서 관찰한 HbA1c의 경우, 두 처치 집단에서 유의한 감소가 나타남과 동시에 아무런 처치도 받지 않은 통제집단 역시 유의하게 감소하였다. 이와 같은 결과를 설명할 수 있는 보고로, WHO(2011)는 HbA1c가 지난 3개월간의 평균 혈중 글루코스를 반영한다고 언급하였으며, Cheon & Koh(2011)는 HbA1c와 신체활동 사이의 부적 상관관계가 있다고 제시하였다. 본 연구의 대상자 선정 시 지난 6개월 간 규칙적인 운동을 수행하지 않은 자만을 포함시키긴 하였으나, 운동량뿐만 아니라 걷기와 같은 신체활동량에 의해서도 HbA1c가 변화될 수 있다고 보고됨에 따라, 일상 중의 신체활동량이 영향을 미쳤을 가능성이 존재한다.
이상에서 전술한 내용을 종합해 보면, 단기간의 HIIT에서도 인슐린 민감성과 인슐린 저항성을 개선하는데 효과적인 것으로 판단된다. 본 연구의 HIIT집단에서 인슐린 저항성 지표가 감소되는 경향이 나타났으나 유의하지 않았던 이유는, 실시한 운동 기간(6주)이 다소 짧았으며, 대상자가 20대인 점으로 인하여 인슐린 저항성과 관련된 기존의 혈액 변인들의 수치가 정상을 유지하고 있었기 때문으로 사료된다. 또한 운동과 함께 식단 조절이나 칼로리 섭취의 제한을 병행하는 것은 체중 조절과 글루코스 대사를 향상시키는데 더욱 큰 효과를 나타낸다고 보고됨에 따라(Dunn et al., 2014) 향후 연구에서는 이상의 내용을 보완하여 6주 이상의 기간 동안 대사증후군 환자나 제2형 당뇨병 환자에게 식단 조절과 함께 HIIT를 실시한다면 인슐린 저항성 개선에 더욱 의미 있는 연구가 될 것으로 판단된다.
혈중 지질의 변화
혈중 지질 중 TG는 지방의 저장 형태이고, LDL-C는 콜레스테롤을 말초 조직으로 운반하는 역할을 하며, HDL-C는 콜레스테롤을 간으로 운반시켜 체외로 배출시킨다. 위와 같은 혈중 지질의 농도가 비정상적으로 변화될 때 이상지질혈증이 발병한다(ACSM, 2013). 이상지질혈증의 증세는 TG 및 LDL-C의 증가와 HDL-C의 감소로 보고되었다(Meshsani & Adeli, 2009).
이 연구의 결과, HIIT와 MICT집단에서 혈중 지질과 관련된 모든 변인이 통계적으로 유의하게 변화하지 않았으나 HDL-C(6.37%, 2.59% 증가)와 TG(21.57%, 5.14% 감소)가 개선되는 경향을 보였으며, 특히 HIIT집단에서 긍정적인 변화가 더욱 뚜렷하게 나타났다. 비슷한 연구 결과로, Heydari et al.(2012)은 과체중의 젊은 남성을 대상으로 12주간 주3회 HIIT를 실시한 결과 통계적으로 유의한 감소가 나타나지 않았으나 LDL-C, HDL-C, TC, 그리고 TG에서 감소되는 경향이 나타났다. 이와 더불어 Durstine et al.(2002)은 유산소 운동을 실시한 대부분의 연구에서 TG와 HDL-C는 향상되었고, 반대로 TC와 LDL-C는 변화가 나타나지 않았다고 보고하여 본 연구의 결과와 유사한 것으로 나타났다. 이와는 상반된 의견으로, Sandvei et al.(2012)은 8주간 HIIT를 실시한 결과 TC와 LDL-C가 유의하게 감소된 반면 HDL-C는 변화되지 않았으며, MICT집단은 세 변인 모두 유의한 변화가 나타나지 않았다고 보고하였다. 또한 Kang(2013)은 내당능장애를 가진 중년 여성을 대상으로 12주간 주5회 HIIT와 MICT를 수행한 결과 두 집단 모두에서 TC와 TG가 유의하게 감소되었으나, LDL-C와 HDL-C의 유의한 변화는 나타나지 않았다고 보고하였다. 이와 같이 상반된 연구 결과가 나타난 이유는 혈중 지질의 성분이 트레이닝 이외에도 개인의 영양 상태, 성별, 연령, 신체구성, 생활습관, 그리고 운동 전 콜레스테롤 수준 등 다양한 요인에 의해서도 조절될 수 있기 때문이라고 사료되며(Durstine & Haskell, 1994), 이에 따라 HIIT의 효과를 명확하게 규명하기 위해서는 가외변인을 최소화한 연구의 추가 수행이 요청된다.
이상의 내용을 종합해 보면, HIIT 처치가 MICT 처치에 비해 TG와 HDL-C의 개선에 효과가 있는 것으로 판단된다. 그러나 감소 경향이 나타났을 뿐, 유의한 변화가 나타나지 않았던 일부 변인들의 경우 20대 남성으로서 실시한 운동 기간(6주)이 다소 짧았으며, 대상자들의 혈중 지질 수준이 매우 정상이었기 때문으로 사료된다. TG의 경우 유산소 운동을 실시한다고 해서 항상 감소하는 것은 아니며, 감소의 정도는 기존 TG의 수준과 관련되어 있다는 Durstine et al.(2002)의 연구를 참고하였을 때 본 연구의 대상자들의 기본적인 TG의 수준이 정상 수준을 유지하고 있는 점 등에 기인한 것으로 사료된다.
결 론
이 연구의 목적은 6주간의 HIIT와 MICT가 20대 과체중 남성의 신체구성, 유산소 운동능력, 심혈관기능, 인슐린 저항성 및 혈중 지질에 미치는 영향을 규명하는 것이었으며, 본 연구에서 얻은 결과를 요약하여 제시하면 다음과 같다.
1) 신체구성과 관련하여, HIIT집단에서 체중, BMI, 체지방량, 그리고 허리-엉덩이둘레비가 유의하게 감소되었다. 2) 유산소 운동능력과 관련하여, VO2max, VEmax, 그리고 최대운동부하검사 시 탈진까지 소요된 시간에서 집단과 시기의 상호작용이 유의하게 나타났으며 다른 두 집단에 비해 HIIT집단에서 유의하게 높은 수준이 나타났다. 3) 심혈관기능과 관련하여, HIIT집단에서만 수축기 혈압이 유의하게 감소되었으며, 안정시 심박수은 통계적으로 유의하지 않았지만 감소되는 경향을 보였다. 4) 인슐린 저항성과 관련된 모든 변인에서 통계적으로 유의한 변화가 나타나지는 않았으나, 공복 인슐린과 HOMA-IR이 HIIT집단에서만 개선되는 경향을 보였다. 5) 혈중 지질의 모든 변인에서 통계적으로 유의한 변화가 나타나지 않았으나, HDL-C와 TG가 HIIT집단에서 개선되는 경향을 보였다.
이상의 결과를 종합해 보면, 6주간의 HIIT 처치가 MICT에 비하여 유산소 운동능력과 심혈관기능의 향상에 더 긍정적인 영향을 미치는 것으로 결론지을 수 있으며, 신체구성, 인슐린 저항성, 그리고 혈중 지질을 개선할 수 있는 가능성이 제시되었다. 향후 HIIT가 MICT에 비하여 효과적인 생화학적 기전을 규명하는 연구가 요청된다.
References
American College of Sports Medicine.(2013). ACSM's Guidelines for Exercise Testing and Prescription.Lippincott Williams and Wilkins: Philadelphia, PA.
American College of Sports Medicine. 2013. ACSM's Guidelines for Exercise Testing and Prescription Lippincott Williams and Wilkins. Philadelphia, PA:American College of Sports Medicine(2015). Predicted Top 10 Fitness Trends.
American College of Sports Medicine. 2015. Predicted Top 10 Fitness TrendsBaster-Brooks, C. & Baster, T.(2005). Exercise and hypertension. Australian Family Physician, 34(6), 419-424.
Baster-Brooks C., et al, Baster T.. 2005;Exercise and hypertension. Australian Family Physician 34(6):419–424.Bilski, J., Teległów, A., Zahradnik-Bilska, J., Dembiński, A., & Warzecha, Z.(2009). Effects of exercise on appetite and food intake regulation. Medicina Sportiva, 13(2), 82-94.
Bilski J., Teległów A., Zahradnik-Bilska J., Dembiński A., et al, Warzecha Z.. 2009;Effects of exercise on appetite and food intake regulation. Medicina Sportiva 13(2):82–94.Boutcher, S. H.(2011). High-intensity intermittent exercise and fat loss. Journal of Obesity, 2011(Article ID: 868305), 1-10.
Boutcher S. H.. 2011;High-intensity intermittent exercise and fat loss. Journal of Obesity 2011(Article ID: 868305):1–10. 10.1155/2011/868305.Bruce, R., Kusumi, F., & Hosmer, D.(1973). Maximal oxygen intake and nomographic assessment of functional aerobic impairment in cardiovascular disease. American Heart Journal, 85(4), 546-562.
Bruce R., Kusumi F., et al, Hosmer D.. 1973;Maximal oxygen intake and nomographic assessment of functional aerobic impairment in cardiovascular disease. American Heart Journal 85(4):546–562. 10.1016/0002-8703(73)90502-4.Brum, P. C., Bacurau, A. V., Cunha, T. F., Bechara, L. R. G., & Moreira, J. B. N. (2014). Skeletal myopathy in heart failure: effects of aerobic exercise training. Experimental Physiology, 99(4), 616-620.
Brum P. C., Bacurau A. V., Cunha T. F., Bechara L. R. G., et al, Moreira J. B. N.. 2014;Skeletal myopathy in heart failure: effects of aerobic exercise training. Experimental Physiology 99(4):616–620. 10.1113/expphysiol.2013.076844.Burgomaster, K. A., Heigenhauser, G. J., & Gibala, M. J.(2006). Effect of short-term sprint interval training on human skeletal muscle carbohydrate metabolism during exercise and time-trial performance. Journal of Applied Physiology, 100(6), 2041-2047.
Burgomaster K. A., Heigenhauser G. J., et al, Gibala M. J.. 2006;Effect of short-term sprint interval training on human skeletal muscle carbohydrate metabolism during exercise and time-trial performance. Journal of Applied Physiology 100(6):2041–2047. 10.1152/japplphysiol.01220.2005.Cheon, K. H. & Koh, K. W.(2011). Relationship between HbA1c and physical activity in korean older adults. Korean Public Health Research, 37(1), 59-71.
Cheon K. H., et al, Koh K. W.. 2011;Relationship between HbA1c and physical activity in korean older adults. Korean Public Health Research 37(1):59–71.Ciolac, E. G.(2012). High-intensity interval training and hypertension: maximizing the benefits of exercise?. American Journal of Cardiovascular Disease, 2(2), 102-110.
Ciolac E. G.. 2012;High-intensity interval training and hypertension: maximizing the benefits of exercise? American Journal of Cardiovascular Disease 2(2):102–110.Collier, S. R., Kanaley, J. A., Carhart Jr, R., Frechette, V., Tobin, M. M., Bennett, N., Luckenbaugh, A. N., & Fernhall, B.(2009). Cardiac autonomic function and baroreflex changes following 4 weeks of resistance versus aerobic training in individuals with pre hypertension. Acta Physiologica, 195(3), 339-348.
Collier S. R., Kanaley J. A., Carhart Jr R., Frechette V., Tobin M. M., Bennett N., Luckenbaugh A. N., et al, Fernhall B.. 2009;Cardiac autonomic function and baroreflex changes following 4 weeks of resistance versus aerobic training in individuals with pre hypertension. Acta Physiologica 195(3):339–348. 10.1111/j.1748-1716.2008.01897.x.Cooney, M. T., Vartiainen, E., Laakitainen, T., Juolevi, A., Dudina, A., & Graham, I. M.(2010). Elevated resting heart rate is an independent risk factor for cardiovascular disease in healthy men and women. American Heart Journal, 159(4), 612-619.
Cooney M. T., Vartiainen E., Laakitainen T., Juolevi A., Dudina A., et al, Graham I. M.. 2010;Elevated resting heart rate is an independent risk factor for cardiovascular disease in healthy men and women. American Heart Journal 159(4):612–619. 10.1016/j.ahj.2009.12.029.Cornelissen, V. A., Buys, R., & Smart, N. A.(2013). Endurance exercise beneficially affects ambulatory blood pressure: a systematic review and meta-analysis. Journal of hypertension, 31(4), 639-648.
Cornelissen V. A., Buys R., et al, Smart N. A.. 2013;Endurance exercise beneficially affects ambulatory blood pressure: a systematic review and meta-analysis. Journal of hypertension 31(4):639–648.Donnelly, J. E., Hill, J. O., Jacobsen, D. J., Potteiger, J., Sullivan, D. K., Johnson, S. L., Heelan, K. Hise, M., Fennessey, P. V., Sonko, B., Sharp, T., Jakicic, J. M., Blair, S. N., Tran, Z. V., Mayo, M., Gibsob, C., & Washburn, R. A.(2003). Effects of a 16-month randomized controlled exercise trial on body weight and composition in young, overweight men and women: the Midwest Exercise Trial. Archives of Internal Medicine, 163(11), 1343-1350.
Donnelly J. E., Hill J. O., Jacobsen D. J., Potteiger J., Sullivan D. K., Johnson S. L., Heelan K., Hise M., Fennessey P. V., Sonko B., Sharp T., Jakicic J. M., Blair S. N., Tran Z. V., Mayo M., Gibsob C., et al, Washburn R. A.. 2003;Effects of a 16-month randomized controlled exercise trial on body weight and composition in young, overweight men and women: the Midwest Exercise Trial. Archives of Internal Medicine 163(11):1343–1350.Dunn, S. L., Siu, W., Freund, J., & Boutcher, S. H.(2014). The effect of a lifestyle intervention on metabolic health in young women. Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy, 19(7), 437-444.
Dunn S. L., Siu W., Freund J., et al, Boutcher S. H.. 2014;The effect of a lifestyle intervention on metabolic health in young women. Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy 19(7):437–444.Durstine, J. L., & Haskell, W. L.(1994). Effects of exercise training on plasma lipids and lipoproteins. Exercise and Sport Sciences Reviews, 22(1), 477-522.
Durstine J. L., et al, Haskell W. L.. 1994;Effects of exercise training on plasma lipids and lipoproteins. Exercise and Sport Sciences Reviews 22(1):477–522.Durstine, J. L., Grandjean, P. W., Cox, C. A., & Thompson, P. D.(2002). Lipids, lipoproteins, and exercise. Journal of Cardiopulmonary Rehabilitation and Prevention, 22(6), 385-398.
Durstine J. L., Grandjean P. W., Cox C. A., et al, Thompson P. D.. 2002;Lipids, lipoproteins, and exercise. Journal of Cardiopulmonary Rehabilitation and Prevention 22(6):385–398.Friedewald, W. T., Robert, I. L., & Donald, S. F.(1972). Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clinical Chemistry, 18(6), 499-502.
Friedewald W. T., Robert I. L., et al, Donald S. F.. 1972;Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clinical Chemistry 18(6):499–502.Gibala, M. J., Little, J. P., Van Essen, M., Wilkin, G. P., Burgomaster, K. A., Safdar, A., Raha, S., & Tarnopolsky, M. A.(2006). Short‐term sprint interval versus traditional endurance training: similar initial adaptations in human skeletal muscle and exercise performance. The Journal of Physiology, 575(3), 901-911.
Gibala M. J., Little J. P., Van Essen M., Wilkin G. P., Burgomaster K. A., Safdar A., Raha S., et al, Tarnopolsky M. A.. 2006;Short‐term sprint interval versus traditional endurance training: similar initial adaptations in human skeletal muscle and exercise performance. The Journal of Physiology 575(3):901–911. 10.1113/jphysiol.2006.112094.Gibala, M. J., Little, J. P., Mac-Donald, M. J., & Hawley, J. A.(2012). Physiological adaptations to low‐volume, high‐intensity interval training in health and disease. The Journal of Physiology, 590(5), 1077-1084.
Gibala M. J., Little J. P., Mac-Donald M. J., et al, Hawley J. A.. 2012;Physiological adaptations to low‐volume, high‐intensity interval training in health and disease. The Journal of Physiology 590(5):1077–1084. 10.1113/jphysiol.2011.224725.Gleser, M. A. & Vogel, J. A.(1971). Endurance exercise: effect of work-rest schedules and repeated testing. Journal of Applied Physiology, 31(5), 735-739.
Gleser M. A., et al, Vogel J. A.. 1971;Endurance exercise: effect of work-rest schedules and repeated testing. Journal of Applied Physiology 31(5):735–739. 10.1152/jappl.1971.31.5.735.Gormley, S. E., Swain, D. P., High, R., Spina, R. J., Dowling, E. A., Kotipalli, U. S., & Gandrakota, R.(2008). Effect of intensity of aerobic training on VO2max. Medicine and Science in Sports and Exercise, 40(7), 1336-1343.
Gormley S. E., Swain D. P., High R., Spina R. J., Dowling E. A., Kotipalli U. S., et al, Gandrakota R.. 2008;Effect of intensity of aerobic training on VO2max. Medicine and Science in Sports and Exercise 40(7):1336–1343. 10.1249/01.mss.0000321629.41403.46.Hansen, D., Dendale, P., Jonkers, R. A. M., Beelen, M., Manders, R. J. F., Corluy, L., Mullens, A., Berger, J., Meeusen, R., & Van Loon, L. J. C. (2009). Continuous low-to moderate-intensity exercise training is as effective as moderate-to high-intensity exercise training at lowering blood HbA1c in obese type 2 diabetes patients. Diabetologia, 52(9), 1789-1797.
Hansen D., Dendale P., Jonkers R. A. M., Beelen M., Manders R. J. F., Corluy L., Mullens A., Berger J., Meeusen R., et al, Van Loon L. J. C.. 2009;Continuous low-to moderate-intensity exercise training is as effective as moderate-to high-intensity exercise training at lowering blood HbA1c in obese type 2 diabetes patients. Diabetologia 52(9):1789–1797. 10.1007/s00125-009-1354-3.Helgerud, J., Hoydal, K., Wang, E., Karlsen, T., Berg, P., Bjerkaas, M., Simonsen, T., Helgesen, C., Hjorth, N., Bach, R., & Hoff, J.(2007). Aerobic high-intensity intervals improve VO2max more than moderate training. Medicine and Science in Sports and Exercise, 39(4), 665-671.
Helgerud J., Hoydal K., Wang E., Karlsen T., Berg P., Bjerkaas M., Simonsen T., Helgesen C., Hjorth N., Bach R., et al, Hoff J.. 2007;Aerobic high-intensity intervals improve VO2max more than moderate training. Medicine and Science in Sports and Exercise 39(4):665–671. 10.1249/mss.0b013e3180304570.Heydari, M., Freund, J., & Boutcher, S. H.(2012). The effect of high-intensity intermittent exercise on body composition of overweight young males. Journal of Obesity, 2012(Article ID: 480467), 1-8.
Heydari M., Freund J., et al, Boutcher S. H.. 2012;The effect of high-intensity intermittent exercise on body composition of overweight young males. Journal of Obesity 2012(Article ID: 480467):1–8. 10.1155/2012/480467.Hickson, R. C., Bomze, H. A., & Holloszy, J. O.(1977). Linear increase in aerobic power induced by a strenuous program of endurance exercise. Journal of Applied Physiology, 42(3), 372-376.
Hickson R. C., Bomze H. A., et al, Holloszy J. O.. 1977;Linear increase in aerobic power induced by a strenuous program of endurance exercise. Journal of Applied Physiology 42(3):372–376. 10.1152/jappl.1977.42.3.372.Hottenrott, K., Ludyga, S., & Schulze, S.(2012). Effects of high intensity training and continuous endurance training on aerobic capacity and body composition in recreationally active runners. Journal of Sports Science and Medicine, 11(3), 483-488.
Hottenrott K., Ludyga S., et al, Schulze S.. 2012;Effects of high intensity training and continuous endurance training on aerobic capacity and body composition in recreationally active runners. Journal of Sports Science and Medicine 11(3):483–488.Jelleyman, C., Yates, T., O'Donovan, G., Gray, L. J., King, J. A., Khunti, K., & Davies, M. J.(2015). The effects of high‐intensity interval training on glucose regulation and insulin resistance: a meta analysis. Obesity Reviews, 16(11), 942-961.
Jelleyman C., Yates T., O'Donovan G., Gray L. J., King J. A., Khunti K., et al, Davies M. J.. 2015;The effects of high‐intensity interval training on glucose regulation and insulin resistance: a meta analysis. Obesity Reviews 16(11):942–961. 10.1111/obr.12317.Jensen, M. D., Ryan, D. H., & Apovian, C. M.(2014). 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults:a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Obesity Society.
Jensen M. D., Ryan D. H., et al, Apovian C. M.. 2014. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults:a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Obesity SocietyJung, S. L., Kim, B. R., & Kang, S. J.(2011). Effects of interval training and aerobic exercise on cardiorespiratory fitness and arterial stiffness in metabolic syndrome patients. The Official Journal of the Korean Academy of Kinesiology, 13(3), 41-52.
Jung S. L., Kim B. R., et al, Kang S. J.. 2011;Effects of interval training and aerobic exercise on cardiorespiratory fitness and arterial stiffness in metabolic syndrome patients. The Official Journal of the Korean Academy of Kinesiology 13(3):41–52.Kang, S. J.(2013). Effects of interval training and aerobic exercise on insulin resistance in middle-aged women with impaired glucose tolerance. The Korean Journal of Physical Education, 52(1), 387-397.
Kang S. J.. 2013;Effects of interval training and aerobic exercise on insulin resistance in middle-aged women with impaired glucose tolerance. The Korean Journal of Physical Education 52(1):387–397.Lau, P. W., Wong, D. P., Ngo, J. K., Liang, Y., Kim, C. G., & Kim, H. S.(2015). Effects of high-intensity intermittent running exercise in overweight children. European Journal of Sport Science, 15(2), 182-190.
Lau P. W., Wong D. P., Ngo J. K., Liang Y., Kim C. G., et al, Kim H. S.. 2015;Effects of high-intensity intermittent running exercise in overweight children. European Journal of Sport Science 15(2):182–190. 10.1080/17461391.2014.933880.Li, N., Fu, J., Koonen, D. P., Kuivenhoven, J. A., Snieder, H., & Hofker, M. H.(2014). Are hypertriglyceridemia and low HDL causal factors in the development of insulin resistance?. Atherosclerosis, 233(1), 130-138.
Li N., Fu J., Koonen D. P., Kuivenhoven J. A., Snieder H., et al, Hofker M. H.. 2014;Are hypertriglyceridemia and low HDL causal factors in the development of insulin resistance? Atherosclerosis 233(1):130–138. 10.1016/j.atherosclerosis.2013.12.013.Matthews, D. R., Hosker, J. P., Rudenski, A. S., Naylor, B. A., Treacher, D. F., & Turner, R. C.(1985). Homeostasis model assessment: insulin resistance and β-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia, 28(7), 412-419.
Matthews D. R., Hosker J. P., Rudenski A. S., Naylor B. A., Treacher D. F., et al, Turner R. C.. 1985;Homeostasis model assessment: insulin resistance and β-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 28(7):412–419. 10.1007/bf00280883.Meshkani, R. & Adeli, K.(2009). Hepatic insulin resistance, metabolic syndrome and cardiovascular disease. Clinical Biochemistry, 42(13), 1331-1346.
Meshkani R., et al, Adeli K.. 2009;Hepatic insulin resistance, metabolic syndrome and cardiovascular disease. Clinical Biochemistry 42(13):1331–1346. 10.1016/j.clinbiochem.2009.05.018.Milanovic, Z., Sporis, G., Weston, M.(2015). Effectiveness of high-intensity interval training(HIT) and continuous endurance training for VO2max improvements: A systematic review and meta-analysis of controlled trials. Sports Medicine, 45(10), 1469-1481.
Milanovic Z., Sporis G., Weston M.. 2015;Effectiveness of high-intensity interval training(HIT) and continuous endurance training for VO2max improvements: A systematic review and meta-analysis of controlled trials. Sports Medicine 45(10):1469–1481.Ministry of Health and Welfare(2013). 2013 Information on Integrated Health Promotion Program for Community.
Ministry of Health and Welfare. 2013. 2013 Information on Integrated Health Promotion Program for CommunityMitchell, G. F.(2014). Arterial stiffness and hypertension. Hypertension, 64(1), 13-18.
Mitchell G. F.. 2014;Arterial stiffness and hypertension. Hypertension 64(1):13–18. 10.1161/hypertensionaha.114.00921.Molmen-Hansen, H. E., Stolen, T., Tjonna, A. E., Aamot, I. L., Ekeberg, I. S., Tyldum, G. A., Wisloff, U., Ingul, C. B., & Stoylen, A.(2012). Aerobic interval training reduces blood pressure and improves myocardial function in hypertensive patients. European Journal of Preventive Cardiology, 19(2), 151-160.
Molmen-Hansen H. E., Stolen T., Tjonna A. E., Aamot I. L., Ekeberg I. S., Tyldum G. A., Wisloff U., Ingul C. B., et al, Stoylen A.. 2012;Aerobic interval training reduces blood pressure and improves myocardial function in hypertensive patients. European Journal of Preventive Cardiology 19(2):151–160. 10.1177/1741826711400512.National High Blood Pressure Education Program(2004). The seventh report of the Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure. JAMA, 289(19), 2560-2572.
National High Blood Pressure Education Program. 2004;The seventh report of the Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure. JAMA 289(19):2560–2572.Nemoto, K. I., Gen-no, H., Masuki, S., Okazaki, K., & Nose, H.(2007). Effects of high-intensity interval walking training on physical fitness and blood pressure in middle-aged and older people. In Mayo Clinic Proceedings, 82(7), 803-811.
Nemoto K. I., Gen-no H., Masuki S., Okazaki K., et al, Nose H.. 2007. Effects of high-intensity interval walking training on physical fitness and blood pressure in middle-aged and older people. In. Mayo Clinic Proceedings 82(7)803–811.Nybo, L., Sundstrup, E., Jakobsen, M. D., Mohr, M., Hornstrup, T., Simonsen, L., Bulow, J., Randers, M. R., Nielsen, J. J., Aagaard, P., & Krustrup, P.(2010). High-intensity training versus traditional exercise interventions for promoting health. Medicine and Science in Sports and Exercise, 42(10), 1951-8.
Nybo L., Sundstrup E., Jakobsen M. D., Mohr M., Hornstrup T., Simonsen L., Bulow J., Randers M. R., Nielsen J. J., Aagaard P., et al, Krustrup P.. 2010;High-intensity training versus traditional exercise interventions for promoting health. Medicine and Science in Sports and Exercise 42(10):1951–8. 10.1249/mss.0b013e3181d99203.Pattyn, N., Coeckelberghs, E., Buys, R., Cornelissen, V. A., & Vanhees, L.(2014). Aerobic interval training vs. moderate continuous training in coronary artery disease patients: a systematic review and meta-analysis. Sports Medicine, 44(5), 687-700.
Pattyn N., Coeckelberghs E., Buys R., Cornelissen V. A., et al, Vanhees L.. 2014;Aerobic interval training vs. moderate continuous training in coronary artery disease patients: a systematic review and meta-analysis. Sports Medicine 44(5):687–700. 10.1007/s40279-014-0158-x.Richards, J. C., Johnson, T. K., Kuzma, J. N., Lonac, M. C., Schweder, M. M., Voyles, W. F., & Bell, C.(2010). Short‐term sprint interval training increases insulin sensitivity in healthy adults but does not affect the thermogenic response to β‐adrenergic stimulation. The Journal of Physiology, 588(15), 2961-2972.
Richards J. C., Johnson T. K., Kuzma J. N., Lonac M. C., Schweder M. M., Voyles W. F., et al, Bell C.. 2010;Short‐term sprint interval training increases insulin sensitivity in healthy adults but does not affect the thermogenic response to β‐adrenergic stimulation. The Journal of Physiology 588(15):2961–2972. 10.1113/jphysiol.2010.189886.Rognmo, Ø., Hetland, E., Helgerud, J., Hoff, J., & Slørdahl, S. A.(2004). High intensity aerobic interval exercise is superior to moderate intensity exercise for increasing aerobic capacity in patients with coronary artery disease. European Journal of Cardiovascular Prevention and Rehabilitation, 11(3), 216-222.
Rognmo Ø., Hetland E., Helgerud J., Hoff J., et al, Slørdahl S. A.. 2004;High intensity aerobic interval exercise is superior to moderate intensity exercise for increasing aerobic capacity in patients with coronary artery disease. European Journal of Cardiovascular Prevention and Rehabilitation 11(3):216–222. 10.1097/01.hjr.0000131677.96762.0c.Sandvei, M., Jeppesen, P. B., Støen, L., Litleskare, S., Johansen, E., Stensrud, T., Enoksen, E., Hautala, A., Martinmaki, K., Kinnunen, H., Tulppo, M., & Jensen, J.(2012). Sprint interval running increases insulin sensitivity in young healthy subjects. Archives of Physiology and Biochemistry, 118(3), 139-147.
Sandvei M., Jeppesen P. B., Støen L., Litleskare S., Johansen E., Stensrud T., Enoksen E., Hautala A., Martinmaki K., Kinnunen H., Tulppo M., et al, Jensen J.. 2012;Sprint interval running increases insulin sensitivity in young healthy subjects. Archives of Physiology and Biochemistry 118(3):139–147. 10.3109/13813455.2012.677454.Slentz, C. A., Tanner, C. J., Bateman, L. A., Durheim, M. T., Huffman, K. M., Houmard, J. A., & Kraus, W. E.(2009). Effects of exercise training intensity on pancreatic β-cell function. Diabetes Care, 32(10), 1807-1811.
Slentz C. A., Tanner C. J., Bateman L. A., Durheim M. T., Huffman K. M., Houmard J. A., et al, Kraus W. E.. 2009;Effects of exercise training intensity on pancreatic β-cell function. Diabetes Care 32(10):1807–1811. 10.2337/dc09-0032.Spina, R. J.(1999). 10 Cardiovascular adaptations to endurance exercise training in older men and women. Exercise and Sport Sciences Reviews, 27(1), 317-332.
Spina R. J.. 1999;10 Cardiovascular adaptations to endurance exercise training in older men and women. Exercise and Sport Sciences Reviews 27(1):317–332. 10.1249/00003677-199900270-00012.Tjønna, A. E., Lee, S. J., Rognmo, Ø., Stølen, T. O., Bye, A., Haram, P. M., Loennechen, J. P., Al-Share, Q. Y., Skogvoll, E., Slordahl, S. A., Kemi, O. J., Najjar, S. M., & Wisløff, U.(2008). Aerobic interval training versus continuous moderate exercise as a treatment for the metabolic syndrome: A pilot study. Circulation, 118(4), 346-354.
Tjønna A. E., Lee S. J., Rognmo Ø., Stølen T. O., Bye A., Haram P. M., Loennechen J. P., Al-Share Q. Y., Skogvoll E., Slordahl S. A., Kemi O. J., Najjar S. M., et al, Wisløff U.. 2008;Aerobic interval training versus continuous moderate exercise as a treatment for the metabolic syndrome: A pilot study. Circulation 118(4):346–354.Tjønna, A. E., Leinan, I. M., Bartnes, A. T., Jenssen, B. M., Gibala, M. J., Winett, R. A., & Wisløff, U.(2013). Low- and high-volume of intensive endurance training significantly improves maximal oxygen uptake after 10-weeks of training in healthy men. PLoS ONE 8(5): e65382. doi: 10.1371/journal.pone.0065382.
Tjønna A. E., Leinan I. M., Bartnes A. T., Jenssen B. M., Gibala M. J., Winett R. A., et al, Wisløff U.. 2013;Low- and high-volume of intensive endurance training significantly improves maximal oxygen uptake after 10-weeks of training in healthy men. PLoS ONE 8(5):e65382. 10.1371/journal.pone.0065382.Trapp, E. G., Chisholm, D. J., & Boutcher, S. H.(2007). Metabolic response of trained and untrained women during high-intensity intermittent cycle exercise. American Journal of Physiology-Regulatory, Integrative and Comparative Physiology, 293(6), 2370-2375.
Trapp E. G., Chisholm D. J., et al, Boutcher S. H.. 2007;Metabolic response of trained and untrained women during high-intensity intermittent cycle exercise. American Journal of Physiology-Regulatory, Integrative and Comparative Physiology 293(6):2370–2375. 10.1152/ajpregu.00780.2006.Trapp, E. G., Chisholm, D. J., Freund, J., & Boutcher, S. H.(2008). The effects of high-intensity intermittent exercise training on fat loss and fasting insulin levels of young women. International Journal of Obesity, 32(4), 684-691.
Trapp E. G., Chisholm D. J., Freund J., et al, Boutcher S. H.. 2008;The effects of high-intensity intermittent exercise training on fat loss and fasting insulin levels of young women. International Journal of Obesity 32(4):684–691. 10.1038/sj.ijo.0803781.Vincent, S., Berthon, P., Zouhal, H., Moussa, E., Catheline, M., Bentué-Ferrer, D., & Gratas-Delamarche, A.(2004). Plasma glucose, insulin and catecholamine responses to a Wingate test in physically active women and men. European Journal of Applied Physiology, 91(1), 15-21.
Vincent S., Berthon P., Zouhal H., Moussa E., Catheline M., Bentué-Ferrer D., et al, Gratas-Delamarche A.. 2004;Plasma glucose, insulin and catecholamine responses to a Wingate test in physically active women and men. European Journal of Applied Physiology 91(1):15–21. 10.1007/s00421-003-0957-5.Whyte, L. J., Gill, J. M., & Cathcart, A. J.(2010). Effect of 2 weeks of sprint interval training on health-related outcomes in sedentary overweight/obese men. Metabolism, 59(10), 1421-1428.
Whyte L. J., Gill J. M., et al, Cathcart A. J.. 2010;Effect of 2 weeks of sprint interval training on health-related outcomes in sedentary overweight/obese men. Metabolism 59(10):1421–1428. 10.1016/j.metabol.2010.01.002.Wilmore, J. H. & Costill, D. L.(2006). Physiology of sport and exercise(3rd ed.). Seoul: Deahanmedia.
Wilmore J. H., et al, Costill D. L.. 2006. Physiology of sport and exercise (3rd ed.)th ed. Seoul: Deahanmedia.Wisløff, U., Støylen, A., Loennechen, J. P., Bruvold, M., Rognmo, Ø., Haram, P. M., Tjønna, A. E., Helgerud, J., Slørdahl, S. A., Lee, S. J., Videm, V., Bye, A., Smith, G. L., Najjar, S. M., Ellingsen, O., & Skjærpe, T.(2007). Superior cardiovascular effect of aerobic interval training versus moderate continuous training in heart failure patients a randomized study. Circulation, 115(24), 3086-3094.
Wisløff U., Støylen A., Loennechen J. P., Bruvold M., Rognmo Ø., Haram P. M., Tjønna A. E., Helgerud J., Slørdahl S. A., Lee S. J., Videm V., Bye A., Smith G. L., Najjar S. M., Ellingsen O., et al, Skjærpe T.. 2007;Superior cardiovascular effect of aerobic interval training versus moderate continuous training in heart failure patients a randomized study. Circulation 115(24):3086–3094.World Health Organization(2011). Use of Glycated Haemoglobin(HbA1c) in Diagnosis of Diabetes Mellitus: Abbreviated Report of a WHO Consultation.
World Health Organization. 2011. Use of Glycated Haemoglobin(HbA1c) in Diagnosis of Diabetes Mellitus: Abbreviated Report of a WHO ConsultationWu, T., Gao, X., Chen, M., & Van Dam, R. M.(2009). Long‐term effectiveness of diet‐plus‐exercise interventions vs. diet‐only interventions for weight loss: a meta‐analysis. Obesity Reviews, 10(3), 313-323.
Wu T., Gao X., Chen M., et al, Van Dam R. M.. 2009;Long‐term effectiveness of diet‐plus‐exercise interventions vs. diet‐only interventions for weight loss: a meta‐analysis. Obesity Reviews 10(3):313–323. 10.1111/j.1467-789x.2008.00547.x.Yang, J. H. & Choi, J. H.(2011). Effects of high-intensity with short-times interval training on body composition, VO2max, oxidative stress in middle-aged obese women. Journal of Sport and Leisure Studies, 45(2), 801-809.
Yang J. H., et al, Choi J. H.. 2011;Effects of high-intensity with short-times interval training on body composition, VO2max, oxidative stress in middle-aged obese women. Journal of Sport and Leisure Studies 45(2):801–809.