카이로프랙틱과 PNF 운동의 복합처치가 앞쪽머리자세 환자 목 부위의 근뼈대계 기능에 미치는 영향
Effects of Combined Treatment of Chiropractic and PNF Exercise on Musculoskeletal Function in Forward Head Posture Patients
Article information
Abstract
이 연구의 목적은 카이로프랙틱과 PNF 운동의 복합처치가 앞쪽머리자세 환자 목 부위의 근뼈대계 기능에 미치는 영향을 규명하는 것이었다. 앞쪽머리자세 환자 30명을 카이로프랙틱 집단(n=10), PNF 운동 집단(n=10), 그리고 카이로프랙틱+PNF 운동 복합처치 집단(n=10)에 무선할당 하였으며, 각 집단별로 일일 25분, 주 3회, 8주간 해당 처치 프로그램에 참여하도록 하였다. 처치 전과 후에 목뼈 정렬상태, 근력과 근지구력, 그리고 관절가동범위를 측정하여 집단 간, 그리고 검사 간에 비교하였다. 그 결과 세 집단 모두에서 모든 종속변인이 유의하게 변화된 것으로 나타났으며, 카이로프랙틱+PNF 운동 복합처치 집단에서 다른 두 집단에 비하여 그 변화의 양상이 더 유의하게 나타났다. 앞쪽머리전위, 목뼈앞굽음각, 그리고 굽힘과 폄 ROM의 경우 카이로프랙틱+PNF 운동 복합처치 집단에서 다른 두 집단과 비교하여 더 유의한 변화가 나타났다. 좌·우측 굽힘 ROM의 경우 카이로프랙틱+PNF 운동 복합처치 집단에서 PNF 운동 집단에 비해 더 유의한 증가가 나타났다. 이상의 결과를 종합하면, 이 연구에서 적용한 카이로프랙틱 처치, PNF 운동 처치, 그리고 두 가지의 복합처치 모두 앞쪽머리자세 환자의 근뼈대계 기능 회복에 긍정적으로 작용하였으며, 특히 카이로프랙틱과 PNF 운동을 복합적으로 처치하는 것이 서로의 단점을 보완함으로써 각각의 단일 처치에 비하여 더 효과적인 것으로 결론지을 수 있다.
Trans Abstract
This study was designed to investigate the effects of combined treatment of chiropractic and PNF exercise on musculoskeletal function in forward head posture patients. Thirty patients volunteered to participate in the study as subjects, and they were divided into one of three groups, i.e., chiropractic group (n=10), PNF exercise group (n=10), and combined treatment of chiropractic and PNF exercise group (C+P group; n=10). Subjects in three groups went through each program for 25 min/session, three times/wk for eight weeks. Cervical alignment, cervical muscular strength and endurance, and cervical range of motion were measured and compared among groups and between pre- and post-test utilizing two-way ANOVA with repeated measures. Main results of the present study were as follows: 1) All variables regarding cervical alignment increased significantly in all three groups. The changes in C+P group were more significant than other two groups. 2) All variables regarding cervical muscular strength and endurance increased significantly in all three groups. 3) All variables regarding cervical range of motion increased significantly in all three groups. The changes in ROM regarding flexion and extension in C+P group were more significant than other two groups. It was concluded that all three treatments applied in this study would be effective for functional recovery of the musculoskeletal function in forward head posture patients. Especially, combination of chiropractic and PNF pattern exercise would be the most effective intervention for the patients.
서 론
목뼈사이원반(cervical intervertebral disc) 장애, 목뼈(cervical vertebra)의 통증, 목뼈의 삠(sprain) 및 긴장, 목 부위의 근육 및 힘줄의 손상, 그리고 목의 후천성 변형과 같은 목뼈질환은 경제활동이 활발한 20~50대에서 매우 높게 나타나고 있으며, 목뼈질환에 기인한 연간 진료비가 약 3,140억원으로 해마다 증가되고 있는 추세이다(Health Insurance Review & Assessment Service, 2014). 앞쪽머리자세의 대표적인 원인으로 PC 및 스마트폰과 같은 영상단말장비(visual display terminal: VDT)의 지속적인 사용을 들 수 있다(Janwantanakul et al., 2012). Kang et al.(2012)은 VDT의 장기간 사용이 근뼈대계(musculoskeletal system) 문제를 야기한다고 보고하였고, Bonney & Corlett(2002)은 부적절한 자세가 목뼈는 물론 주변 구조물의 손상을 유발할 수 있다고 주장하였다. 앞쪽머리자세의 경우 긴머리근(longus capitis) 및 긴목근(longus colli)과 같은 깊은 목굽힘근(deep cervical flexor muscles)의 약화가 나타나고, 깊은 목굽힘근의 근력과 근지구력의 약화는 목의 통증을 유발하며, 비정상적인 목뼈굽음(cervical cuvature)의 원인이 된다(Jull, 2000). 또한, Häkkinen et al.(2007)은 상체의 근육에서 나타나는 불균형적인 패턴으로 인한 목뼈의 이상 증상이 목뼈 관절가동범위의 저하를 초래한다고 보고하였다. 따라서 앞쪽머리자세 환자에게 있어서 삶의 질과 업무 효율성의 향상을 도모하기 위해서는 발병 이전의 안정적인 척추 배열상태 확보, 그리고 목 부위의 근력, 근지구력 및 관절가동범위의 증진이 필요할 것으로 판단된다.
목뼈 이상 및 질환을 개선하기 위한 방법으로 침(acupuncture) 치료(Que et al., 2013), 신장운동(Yoo, 2013), 카이로프랙틱 요법(Ogura et al., 2011), 그리고 고유수용성신경근촉진법(Kofotolis & Kellis, 2006) 등에 대한 다양한 연구가 국내·외에서 수행되어 왔다. 이 중 카이로프랙틱은 질환의 근본적인 원인을 찾아 치료하는 수기요법으로서, 척추와 골반을 중심으로 교정하여 신체의 운동역학적 기능을 향상시키는 중재방법이다(Dishman et al., 2002). 카이로프랙틱의 원리는 전위된 척추를 교정하여 운동성을 정상적으로 변화시키고 주위의 신경활동을 원활하게 함과 동시에 뼈대근들의 균형을 조절하여 건강한 신체로 회복시키는 것이다(Coulter et al., 2002). 또한, 관절의 가동성을 증가시키고(Morningstar, 2006), 근육의 긴장을 완화하여 불균형적인 상태를 회복하는데 매우 효과적이라고 보고되었다(Korr, 1995).
그러나 카이로프랙틱은 효과적인 처치임에도 불구하고 그 효과가 오래 지속되지 않는다는 단점을 내포하고 있다. 인체는 고유수용기로부터 받은 정보를 바탕으로 신체 정렬 및 주위 환경과의 관계 설정에 관한 상황을 실시간으로 뇌에 전달한다(Gjelsvik, 2008). 그러나 나쁜 자세로 인한 연부조직의 변성은 고유수용성 감각을 손상시킬 수 있다(Brumagne et al., 1999). 그러므로 변위가 나타난 부분을 교정하였음에도 불구하고 재발하는 이유는 교정으로 인한 뼈대의 변화에도 변성된 연부조직 등이 민감하게 반응할 수 없기 때문이다.
따라서 카이로프랙틱의 단점을 보완할 수 있는 방법이 필요하며, 그 대표적인 방법으로 고유수용성신경근촉진법(proprioceptive neuromuscular facilitation: PNF)을 들 수 있다. PNF 운동은 소아마비와 다발성 경화증 이후의 장애를 극복하기 위한 노력의 일환으로 개발된 운동치료법으로서 근뼈대계 질환과 신경계 질환의 치료에 사용되어 왔으며, 다양한 임상 분야에서 그 효과성이 입증되어 왔다(Gabriel et al., 2006). PNF의 원리는 고유수용기를 자극하여 그 기능을 향상시키는 것으로서 여러 가지 패턴을 동시에 적용하는 경우 더욱 효과적으로 고유수용성 감각, 근력, 그리고 관절가동범위를 향상시킨다(Funk et al., 2003).
전술한 내용을 종합하여 보면, 카이로프랙틱은 신체의 운동역학적 기능과 뼈대근의 균형능력 향상에 효과적이고, PNF 운동은 근력과 관절가동범위의 향상에 효과적이며 다양한 임상 분야에서 그 효과성이 입증되어 왔기 때문에, 중재효과를 극대화하기 위해서는 척추의 교정을 위한 카이로프랙틱과 연부조직의 고유수용성 감각을 증진시킬 수 있는 PNF 운동을 병행하는 것이 보다 효과적일 것으로 판단된다. 그러나 카이로프랙틱에 더하여 고유수용성 감각을 향상시킬 수 있는 치료적 운동을 병행하여 실시한 복합처치의 효과를 규명한 연구가 매우 부족한 실정이다. 허리뼈(lumbar vertebra) 교정과 다른 중재를 복합하여 진행된 연구(Kim & Khil, 2010)가 수행되었으나, 목뼈에 대한 카이로프랙틱과 다른 유형의 중재를 병행한 연구는 매우 미흡한 실정이다. PNF 운동의 경우 주로 신경계 손상환자에게 적용되어 왔으며(Oh et al., 2011), 척추의 문제에 적용한 연구는 주로 허리통증에 국한되어 수행되었다(Jeon, 2013). 국외의 경우에는 신경계 손상에 관한 연구(Ribeiro et al., 2013) 및 관절 손상과 관련된 연구(Rubini et al., 2011) 등이 다양하게 수행되었으나, 척추질환에 대한 연구는 국내와 마찬가지로 허리통증에 국한되어 수행되었다(Huang et al., 2014).
교정을 통하여 신체의 운동역학적 기능과 근육의 균형능력을 향상시키는 카이로프랙틱과 고유수용기를 자극하여 근육의 신경지배 기능을 증진시킬 수 있는 PNF 운동의 복합처치는 앞쪽머리자세 환자의 근뼈대계 기능의 개선에 상승효과를 낼 것으로 기대된다. 그러나 지금까지 앞쪽머리자세 환자의 기능 회복을 위하여 카이로프랙틱과 PNF 운동을 병행하여 적용한 연구가 거의 전무한 실정이다. 따라서 이 연구에서는 카이로프랙틱 단일 처치, PNF 운동 단일 처치, 그리고 카이로프랙틱과 PNF 운동을 병행하여 실시한 복합처치가 앞쪽머리자세 환자의 목뼈 정렬상태, 그리고 목 부위의 근력, 근지구력 및 관절가동범위에 미치는 영향을 규명하고자 하였다.
연구방법
연구 대상자
이 연구의 대상자는 K도 P시에 소재한 L사의 사무직 근로자로서 X-ray 판독 결과 앞쪽머리전위(forward head displacement)가 15 ㎜ 이상인 자를 선정하였다(Harrison et al., 1996). 선정 과정에서 정형외과 및 영상의학과 전문의의 소견 상 목뼈의 발달불능, 발달정지, 부골(accessory bone)의 발달, 그리고 비대칭적 구조의 발달 등 목뼈기형(cervical spine anomalies)으로 인하여 이 연구에서 실시하는 처치 적용에 문제가 있는 자, 척추수술을 하였거나 척추부위의 특별한 질환이 있는 자, 그리고 관련 약물을 복용하는 자는 대상자에서 제외시켰다. 선정된 35명을 카이로프랙틱 집단(12명), PNF 운동 집단(12명), 그리고 카이로프랙틱+PNF 운동 복합처치 집단(11명)에 무선할당 하였다. 연구의 진행과정에서 카이로프랙틱 집단의 경우 이사와 통증의 이유로 2명, PNF 운동 집단의 경우 이직과 결혼의 이유로 2명, 그리고 카이로프랙틱+PNF 운동 복합처치 집단의 경우에는 가족계획으로 1명이 탈락하여, 각 집단 별 10명씩 총 30명의 결과만을 최종 분석에 포함시켰다. 연구의 목적과 실험 절차에 대하여 연구자로부터 충분한 설명을 들은 후, 자발적으로 참여하고자 하는 대상자로 부터 검사 동의서를 받은 후 이 연구에 참여시켰다. 연구 대상자의 신체적 특성은 <Table 1>에 제시된 바와 같다.

Physical characteristics of subjects
측정 항목과 방법
체격
신장과 체중을 Lohman et al.(1992)의 방법에 따라 측정하였으며, 신체질량지수(body mass index: BMI)를 체중/신장²(㎏/㎡)의 공식에 의해 산출하였다.
목뼈 정렬상태
목뼈의 정렬상태를 평가하기 위하여 영상의학과에 X-ray 촬영을 의뢰하였다. 대상자를 상체의 근육들을 이완시키고 자연스럽게 선 자세를 취하게 한 후 정면을 바로 응시하게 한 상태에서 단순측면사진(lateral view)을 획득하였다(Harrison et al., 2003b). X-ray 촬영장비(Distal X-ray TITAN 2000, GEMSS Inc., 한국)는 동일한 방사선사의 의해서 운용 및 촬영되었으며, 8주 후에 재촬영을 통하여 목뼈의 정렬상태의 변화를 관찰하였다. 단순측면사진 영상을 토대로 앞쪽머리전위(forward head displacement: FHD)와 목뼈앞굽음각(cervical lordosis angle: CLA)을 측정하였다. FHD는 제2번 목뼈 의 후상방 모서리면과 제7번 목뼈의 후하방 모서리면과의 수평거리로 측정하였다(Harrison et al., 1996). CLA는 CLA는 고리뼈 전·후 돌기를 연결한 선의 직각과 제7번 목뼈 하면을 연하는 선의 직각이 서로 이루는 각으로 측정하였다(Yochum & Rowe, 2005). FHD와 CLA를 측정하는 방법은 각각 <Fig. 1>과 <Fig. 2>에 제시된 바와 같다.

Measurement of FHD
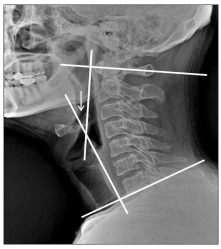
Measurement of CLA
근력과 근지구력
목 부위의 근력과 근지구력을 평가하기 위하여 압력 바이오피드백 장비(Stabilizer Pressure Biofeedback Muscle Testing Device, Chattanooga Inc., 미국)를 이용해서 깊은 목굽힘근(deep cervical flexor muscles)의 최대근력(maximum muscular strength: MMS)과 최대근력의 50% 유지시간(50% of maximum muscular strength maintaining time: 50% MMSM)을 측정하였다. 대상자가 머리를 들지 않은 상태에서 턱을 당기며 머리를 끄덕일(cervical retraction) 때 MMS(㎜Hg)를 측정하였으며, 50%MMSM의 경우 MMS의 50% 압력을 기준으로 유지하는 시간을 초 단위로 기록하였다. MMS를 측정할 때 측정 간에 1분의 휴식시간을 주고 총 5번을 측정하여 가장 높은 값을 선정하였다. 50%MMSM의 경우 측정 전 5분의 휴식시간을 두고 측정하였으며, 측정 간 50%MMSM에서 2㎜Hg의 오차가 발생하게 되면 중단하고 그 시점의 시간을 기록하였다(O’Leary et al., 2007).
관절가동범위
관절가동범위(range of motion: ROM)는 목뼈측각기(cervical range of motion instrument: CROMI, PAINT Inc., 미국)를 이용하여 Norkin & White(2009)가 제시한 방법에 따라 측정하였으며, 목뼈의 굽힘(flexion)과 폄(extension), 좌·우측 굽힘, 그리고 좌·우측 회전 시 ROM을 각각 2회씩 측정하여 높은 값을 기록하였다. 측정을 위하여 목뼈측각기를 대상자의 머리와 코에 조심스럽게 위치시키고, 장비를 알맞게 착용 할 수 있도록 치수조절이 가능한 밴드를 이용하여 고정하였다. 연구자는 측정 오차를 최소화 하고 정확한 동작에서 측정이 가능하도록 대상자의 움직임을 보조하였다. 이 측정방법의 급내상관계수(intra-class correlation coefficients; ICC)는 .88~.99로 보고된 바 있다(Olson et al., 2000).
처치 프로그램
이 연구에서 적용한 처치 프로그램은 ① 카이로프랙틱 처치, ② PNF 운동, 그리고 ③ 카이로프랙틱과 PNF 운동 복합처치였으며, 각 집단에서 일일 25분, 주 3회, 총 8주간 24회의 처치를 동일하게 적용하였다. 카이로프랙틱은 수동적 처치이고 PNF 운동은 능동적 처치였기 때문에 3가지 처치의 총량을 동질화 시키는데 어려움이 있었다. 이 문제점을 극복하기 위하여 준비처치와 정리처치의 시간을 조정하여 각 처치의 총시간을 25분으로 동일하게 구성하였다.
카이로프랙틱 처치
준비처치로 목뼈에서 가동성이 가장 결여된 부분을 찾아 리스팅(listing)을 결정하였으며, 목 부위의 긴장 완화를 위하여 Kaltenborn et al.(2009)의 방법에 근거하여 도수견인(manual traction)을 실시하였다. 정리처치의 경우 도수견인과 목 부위 관절가동범위 운동을 실시하였다. 본처치에서는 목뼈의 교정을 위하여 Modified rotary break를 적용하였다. 대상자의 제 1번 목뼈의 척추몸통(vertebral body)이 오른쪽으로 변위(body right)된 경우(왼쪽으로 변위된 경우에는 오른쪽과 왼쪽이 바뀜) 연구자는 대상자의 오른쪽에 위치하여 연구자의 우측 집게손가락 두 번째와 세 번째 관절의 가쪽을 대상자의 제 1번 목뼈 우측 가로돌기 후면(posterior aspect of the right atlas transverse)에 접촉하였으며, 연구자의 좌측 중지 첫 번째와 두 번째 관절의 전면을 대상자의 뒤통수뼈 왼쪽 후면(left posterior aspect of the occiput)에 접촉하였다. 대상자의 제 2번 목뼈의 척추몸통이 오른쪽으로 변위된 경우 대상자의 제 2번 목뼈의 우측 척추뼈고리판과 척추뼈고리뿌리의 결합부(lamina pedicle junction)와 제 1번 목뼈 좌측 가로돌기 후면에 접촉하였다. 대상자의 세 번째에서 여섯 번째 추체가 오른쪽으로 변위된 경우 변위된 목뼈의 우측 척추뼈고리판과 척추뼈고리뿌리의 결합부와 변위된 목뼈의 바로 위 목뼈(제 3번 목뼈를 교정할 경우에는 제 2번 목뼈가 해당)의 척추뼈고리판과 척추뼈고리뿌리의 결합부에 접촉하였다. 정확한 위치에 접촉을 완료하면 대상자의 목뼈를 뒤에서 앞으로 폄, 아래에서 위로 가쪽굽힘(제 1번 목뼈 교정의 경우, 위에서 아래로 가쪽굽힘), 그리고 오른쪽에서 왼쪽으로 회전시키며 교정하였다(Bergmann & Peterson, 2011). 카이로프랙틱 처치는 카이로프랙틱과 같은 도수교정(manipulation)을 전문적으로 시행하는 의료기관에서의 임상경력이 5년 이상인 물리치료사에 의해 진행되었다. 카이로프랙틱 처치 프로그램은 <Table 2>에 제시된 바와 같다.

Chiropractic therapy program (Modified rotary break)
PNF 운동
준비운동과 정리운동 시간에 전술한 도수견인과 목 부위 관절가동범위 운동을 5분씩 실시하였다. 본운동은 팔의 대칭패턴(symmetrical pattern)과 대칭적 대응패턴(symmetrical-reciprocal pattern)을 적용하여 15분간 진행되었으며, 율동적 개시(rhythmic initiation: RI)와 등장성 수축의 결합(combination of isotonic: CI) 테크닉을 이용하였다(Adler et al., 2008). PNF 운동의 중재는 기본국제코스(International PNF Association Basic Course)를 이수하고 5년 이상의 임상경험이 있는 물리치료사에 의해 진행되었다. PNF 운동 프로그램은 <Table 3>에 제시 된 바와 같다.

PNF exercise program (Upper extremity pattern)
카이로프랙틱+PNF 운동 복합처치
준비처치는 카이로프랙틱 처치 프로그램과 동일하였으나 도수견인의 비중을 축소하여 시간을 10분에서 5분으로 조정하였다. 정리처치의 경우 도수견인과 목 부위 관절가동범위 운동을 5분간 실시하였다. 본처치는 카이로프랙틱과 PNF 운동으로 구성되었다. 카이로프랙틱은 카이로프랙틱 처치 프로그램과 동일한 동작으로 5분간 실시하였고, PNF 운동의 경우 PNF 운동 프로그램과 동일한 방법으로 10분간 실시하였다. 카이로프랙틱+PNF 운동 복합처치 프로그램은 <Table 4>에 제시된 바와 같다.

Combined program of chiropractic therapy and PNF exercise
자료처리 방법
이 연구에서 얻은 자료를 SPSS PC⁺ for Windows (version 21.0)로 분석하였다. 각 집단에서 얻은 검사별 종속변인의 기술통계량을 제시하기 위하여 평균(mean)과 표준편차(standard deviation of mean: SD)를 산출하였다. 세 집단(카이로프랙틱 집단, PNF 운동 집단, 카이로프랙틱+PNF 운동 복합처치 집단) 간, 그리고 두 검사(사전검사, 사후검사) 간 종속변인의 평균 차이를 분석하기 위하여 반복이 있는 이원변량분석(repeated two-way ANOVA)을 실시하였다. 집단과 검사의 주효과 또는 상호작용이 유의한 경우, 동일 검사 내 세 집단 간 평균 차이를 분석하기 위하여 일원변량분석을, 그리고 동일 집단 내 두 검사 간 평균 차이를 분석하기 위하여 종속 t-검증을 실시하였다. 모든 통계적인 유의수준(α)을 .05로 설정하였다.
연구 결과
목뼈 정렬상태
8주간의 세 가지 처치에 따른 목뼈 정렬상태의 변화는 <Table 5>에 제시된 바와 같다. FHD에서 검사의 주효과(P<.001) 및 집단과 검사의 상호작용(P<.01)이 유의하게 나타났으며, CLA에서는 집단의 주효과(P<.05), 검사의 주효과(P<.001), 그리고 집단과 검사의 상호작용(P<.001)이 유의하게 나타났다.

Cervical alignment
(Mean±SD)
카이로프랙틱 집단, PNF 운동 집단, 그리고 복합처치 집단 모두 처치 전과 비교하여 FHD가 유의하게 감소되고 CLA가 유의하게 증가되었다. 특히, 복합처치 집단에서 다른 두 집단과 비교하여 더 유의한 변화가 나타났다.
근력과 근지구력
8주간의 세 가지 처치에 따른 목 부위 근력과 근지구력의 변화는 <Table 6>에 제시된 바와 같다. 근력과 근지구력 모두에서 검사의 주효과(P<.001) 및 집단과 검사의 상호작용(MMS: P<.01; 50% MMSM: P<.05)이 유의하게 나타났다.

Cervical muscle strength and endurance
(Mean±SD)
카이로프랙틱 집단, PNF 운동 집단, 그리고 복합처치 집단 모두 처치 전과 비교하여 MMS와 50% MMSM이 유의하게 증가되었다. 그러나 집단 간에는 처치전과 후에 유의한 차이는 없었다.
관절가동범위
8주간의 세 가지 처치에 따른 관절가동범위의 변화는 <Table 7>에 제시된 바와 같다. ROM관련 모든 변인에서 검사의 주효과(P<.001) 및 집단과 검사의 상호작용(굽힘과 폄: P<.001, 좌ㆍ우측 굽힘 및 좌ㆍ우측 회전: P<.01)이 유의하게 나타났다.

Cervical ROM
(Mean±SD)
카이로프랙틱 집단, PNF 운동 집단, 그리고 복합처치 집단 모두에서 처치 전에 비하여 ROM관련 모든 변인이 유의하게 증가되었다. 특히, 굽힘과 폄 ROM의 경우 복합처치 집단에서 다른 두 집단과 비교하여 더 유의한 변화가 나타났고, 좌·우측 굽힘 ROM의 경우 복합처치 집단에서 PNF 운동 집단에 비해 더 유의한 증가가 나타났다.
논 의
목뼈 정렬상태
이 연구에서는 목뼈의 정렬상태를 평가하기 위하여 앞쪽머리전위(forward head displacement: FHD)와 목뼈앞굽음각(cervical lordosis angle: CLA)을 측정하였다. Harrison et al.(1994)은 목 부위 견인 및 카이로프랙틱 집단, 카이로프랙틱 집단, 그리고 통제 집단으로 나누어 12주간 주 5회 처치한 결과 목 부위 견인 및 카이로프랙틱 집단에서 FHD가 유의하게 변화되었다고 보고하였고, Oh et al.(2014)은 앞쪽머리자세 환자를 대상으로 4주간의 목 부위 관절가동술(mobilization of joint)을 적용한 결과 FHD가 22.6 ㎜에서 18.6 ㎜로 유의하게 감소되었다고 보고하여 이 연구의 결과와 일치하였다. Pearson & Walmsley(1995)는 정상인을 대상으로 목 들임운동(retraction)을 적용하여 중립자세(neutral resting posture)를 평가한 결과, 척추와 귀의 귀구슬(tragus) 사이의 거리가 유의하게 감소되었다고 보고하여, FHD에 대한 즉각적인 교정 효과의 가능성을 제시하였다.
Kim & Kim(2008)은 일자목 환자를 대상으로 주 3회, 16주간의 카이로프랙틱, 스포츠마사지, 그리고 스트레칭을 적용한 결과 CLA가 유의하게 변화되었다고 보고하였으며, Oh et al.(2009)은 목 부위 통증을 호소하는 환자를 대상으로 주 2회, 8주간 봉추나요법과 침요법을 적용한 결과 CLA가 유의하게 개선되었다고 보고하여 이 연구의 결과와 일치하였다. 또한 Harrison et al.(2003a)은 목 부위 통증이 있는 환자를 대상으로 14주간 38회의 카이로프랙틱 견인과 교정을 처치한 결과 CLA가 유의하게 향상되었다고 보고하여 이 연구의 결과와 유사하였다. 반면, Shin et al.(2008)는 목 부위 통증이 있는 근로자를 대상으로 머리-목 굽힘(craniocervical flexion)운동과 목 굽힘(cervical flexion)운동을 6주간 시행한 결과 CLA가 유의하게 변하지 않았다는 이 연구와 다른 결과를 보고하였다. CLA와 관련된 선행연구를 종합해 보면, CLA의 유의한 변화를 도출하기 위해서는 8주 이상의 지속적인 중재가 필요할 것으로 판단된다.
이 연구의 세 집단에서 FHD과 CLA가 개선된 결과가 나타난 이유를 해석하면 다음과 같다. 먼저, 카이로프랙틱 집단의 경우 목뼈 교정을 통하여 틀어진 목뼈의 정상적인 위치가 확보됨에 따라 관절을 구성하는 작용근(agonist), 대항근(antagonist), 그리고 협동근(synergist) 사이의 상호작용으로 인하여 근육의 균형능력이 향상된 것으로 판단된다. 근육의 균형은 신경학적 요소, 뼈대근 요소, 그리고 생역학적 요소에 의해 좌우되며(Gjelsvik, 2008), 목뼈가 정상적인 위치로 변화됨에 따라 뼈대의 정렬, 구조, 그리고 관절의 기능과 같은 생역학적 요소에 적극적으로 반영되어 근육의 불균형이 일정 부분 해소된 것으로 사료된다.
PNF 패턴 운동은 자세 반사의 촉진, 중력을 이용한 동작수행능력의 향상, 원심성 수축에 의한 작용근 활동의 증진, 그리고 대각선 운동 패턴을 통한 두 관절근육의 활성화에 도움을 준다. 따라서 PNF 운동 집단의 경우 팔의 복합패턴을 통하여 어깨의 가동성 증진과 근력의 향상 및 몸통 위를 구성하는 근육의 움직임 및 활성도가 개선된 것으로 판단된다. 또한, 이로 인하여 목뼈를 비롯한 척추 전체의 압력이 감소되고, 몸통의 조절 및 균형능력이 향상되어 목뼈와 등뼈(thoracic vertebra)의 정렬상태에 긍정적인 영향을 미친 것으로 해석할 수 있다. 패턴을 수행할 때 시선에 따른 목의 움직임은 목의 깊은곳에서 오랫동안 신장되어 약해져 있는 긴머리근 및 긴목근을 자극하여 뼈대근의 근섬유 사이 또는 근섬유 내에 평행으로 부착되어 있는 고유수용기인 근방추의 활동을 촉진시켰으며, 긴장성 근수축을 유지하는데 중요한 역할을 하는 감마운동신경원(γ-motor neuron)의 활성도를 증가시켜 목의 깊은 곳에 위치한 근육의 적절한 긴장도 유지에 도움을 주었던 것으로 보인다. 깊은 목굽힘근의 긴장도가 정상적으로 회복되어 적절한 근육의 길이가 확보되었고, 이는 정상적인 목의 동작과 기능을 수행하는데 도움을 주었으며, 이상의 여러 가지 긍정적인 변화는 근육의 불균형 개선과 함께 목뼈의 정상적인 정렬상태에 영향을 미치게 되어 FHD와 CLA의 긍정적 변화를 유도한 것으로 판단된다.
카이로프랙틱+PNF 운동 복합처치 집단의 경우 카이로프랙틱 교정을 통하여 목 부위의 생역학적 요소가 개선되고 근육 균형능력이 촉진되어 목뼈가 정상적인 정렬상태로 회복되었으며, 이에 더하여 PNF 운동을 병행함에 따라 관절의 가동성이 향상되고 깊은 목 근육이 자극되며 척추에 연결된 연부조직의 고유수용감각이 향상되어 다른 두 집단에 비하여 목뼈 정렬상태가 더욱 좋아진 것으로 판단된다.
목 부위 질환의 개선을 위한 처치와 중재관련 선행연구를 살펴보면, 그 처치 방법이 크게 수동적 처치(Ogura et al., 2011; Que et al., 2013)와 능동적 처치(Kofotolis & Kellis, 2006; Yoo, 2013)로 구분되며, 각각 단일 처치의 효과를 규명하는 연구는 있었지만, 이 연구에서와 같이 수동적 처치와 능동적 처치의 복합처치 효과를 분석한 연구는 거의 전무하였다. 이 연구는 카이로프랙틱과 PNF 운동의 복합처치가 앞쪽머리자세 환자의 목뼈 정렬상태의 회복에 가장 효과적이라는 것을 밝혔다는 점에서 의미가 있다고 사료되며, 향후 현장에서 복합처치가 적극적으로 활용되기를 기대한다.
근력과 근지구력
Ylinen et al.(2004)은 목의 통증을 가진 근로자가 건강한 근로자에 비하여 목의 등척성 근력이 유의하게 낮았다고 보고하였고, 목 통증 환자의 재활을 위해서 근력과 근지구력을 향상시킬 수 있는 프로그램이 필요하다고 주장하면서 목 통증의 감소를 위한 근력과 근지구력의 중요성을 강조하였다. Falla et al.(2007)는 깊은 목굽힘근의 근력과 근지구력 향상이 목 부위의 통증을 경감시켜 목뼈의 정상적인 정렬상태로 회복하는데 도움을 줄 수 있다고 보고하였다. 또한, Kim et al.(2007)은 목의 통증을 호소하는 남성 근로자와 건강한 남성 근로자를 대상으로 깊은 목굽힘근의 근력과 근지구력 및 아래턱의 위치 변화를 평가한 결과 통증을 호소하는 집단에서 건강한 집단에 비하여 목의 근력과 근지구력이 유의하게 감소되어 있는 것을 확인하였으며, 아래턱의 위치 변화를 통하여 통증으로 인한 목 부위 근력의 약화가 앞쪽머리자세에 영향을 미칠 수 있다고 주장하였다.
Shin et al.(2008)은 목과 어깨의 통증을 호소하는 사무직 근로자가 머리-목 굽힘운동과 목 굽힘운동을 주 5회, 6주간 실시한 결과 두 처치 모두 목 부위의 근력과 근지구력이 유의하게 향상되었다고 보고하였다. Gong et al.(2010)은 건강한 대학생을 목뼈 관절가동술 집단, 목뼈 안정화운동 집단, 그리고 통제 집단으로 구분하여 주 3회, 3주간 처치를 한 결과 목뼈 관절가동술 집단과 목뼈 안정화운동 집단에서 목 부위의 최대근력과 정적 근지구력이 유의하게 향상되었다고 보고하여 이 연구의 결과와 일치하였다. 또한 Kim et al.(2011)은 목 부위 통증 및 팔의 방사통을 호소하는 사무직 근로자를 대상으로 카이로프랙틱 요법과 슬링을 이용한 견인을 주 2회, 6주간 처치한 결과 목 폄 근력이 유의하게 증가된 것을 확인하였으며, Lee et al.(2014)은 제조업 근로자를 대상으로 6주간 PNF 패턴 운동을 적용한 결과 근활성도가 유의하게 증가되었다고 보고하여 이 연구와 유사한 결과를 보였다.
이 연구에서 실시한 카이로프랙틱 처치는 목뼈의 정상적인 위치를 회복하고 목 부위의 구조 및 관절의 기능과 정렬상태의 정상화에 기여하여 안정적인 척추의 굽음을 형성하는데 도움을 준 것으로 사료된다. 목뼈의 구조적인 개선은 근육의 정상적인 길이 확보에 직접적인 원인으로 작용하였을 뿐만 아니라 근방추의 민감도를 향상시켜 작용근과 대항근의 협력수축을 위한 근육의 균형능력의 증진 및 근육의 동원능력과 반응속도의 증가로 이어져 근력과 근지구력의 향상에 긍정적으로 작용한 것으로 판단된다.
PNF 운동 집단의 경우 카이로프랙틱 집단과 비교하여 목 부위 근력과 근지구력이 더 크게 증가된 경향이 나타났다. PNF 운동 집단에서 실시한 복합패턴을 통한 운동은 시상면, 관상면, 그리고 수평면을 중심으로 움직이는 대각선상의 대단위 운동으로 일어나며, 결합된 기능적인 운동이 몸통의 안정성과 함께 고유수용성 감각과 근력의 향상에 기여한 것으로 판단된다. 이 연구에서 복합패턴 운동을 실시하는 동안 직접적으로 운동을 실시하지 않았던 부위의 근력을 향상시키는 교차훈련의 효과가 더욱 크게 작용하였으며, 점진적인 운동 횟수의 증가 및 PNF의 테크닉 중 하나인 CI 사용은 몸통의 안정성 향상에 긍정적으로 작용함과 동시에 목의 움직임을 촉진시켜 근력을 향상시키는데 도움이 된 것으로 판단된다. 특히, 패턴에서 적용된 CI 테크닉은 팔의 등척성 운동을 촉진하였고 저항을 통한 방산(irradiation) 효과를 가져와 몸통을 비롯하여 척추 및 목 부위 근육의 등척성 근력을 향상시킨 것으로 사료된다. 이에 더하여 골지건기관과 같은 고유수용기는 뼈대근의 장력 변화를 감지하여 중추신경계에 정보를 전달하는데, 근방추와 마찬가지로 골지건기관은 근 수축이 동반된 능동적인 동작에 더욱 활성화되기 때문에(Gjelsvik, 2008) PNF 운동이 근력과 근지구력에 긍정적인 영향을 미친 것으로 사료한다. 이 연구에서 도출된 결과와 같이 목 부위 질환의 문제를 해결하기 위해서는 수의적인 근육 수축이 중요하다고 판단되며, 이는 관련 선행연구(Hoving et al., 2002)를 통해서 뒷받침된다.
한편, 카이로프랙틱+PNF 운동 복합처치 집단의 경우 먼저 카이로프랙틱 처치로 인하여 목 부위의 생역학적 요소가 개선되어 정상적인 목뼈의 해부학적 배열이 확보된 상태에서 PNF 운동이 진행되었기 때문에 근육 내의 고유수용기가 더욱 활성화 되고 효율적이면서 안정적인 운동의 실시가 가능했을 것으로 판단된다. 이를 통하여 단일 처치에 비하여 근력과 근지구력의 향상이 더욱 두드러지는 시너지 효과가 나타난 것으로 보인다.
관절가동범위
Youdas et al.(1992)은 11~97세의 건강한 남녀 337명을 대상으로 목뼈 ROM을 측정하여 30대의 경우 평균 ROM이 폄 73.1°, 좌측 굽힘 42.4°, 우측 굽힘 44.7°, 좌측 회전 65.6°, 그리고 우측 회전이 69.4°라고 보고하였으며, Lantz et al.(1999)은 20~39세의 평균 목뼈 ROM이 굽힘 60°, 폄 58°, 좌측 굽힘 41°, 우측 굽힘 43°, 좌측 회전 73°, 그리고 우측 회전이 72°라고 보고하였다. 국내의 경우 20대 정상인 남녀 100명을 기준으로 평균 목뼈 ROM이 굽힘 55.0°, 폄 70.3°, 좌측 굽힘 43.4°, 우측 굽힘 41.2°, 좌측 회전 67.9°, 그리고 우측 회전이 67.3°라고 보고된 바 있다(Kwon et al, 2010). 이상의 결과를 종합해 보면, 목뼈 ROM의 정상범위가 굽힘 55.0~60.0°, 폄 58.0~ 73.1°, 좌측 굽힘 41~43.4°, 우측 굽힘 41.2~44.7°, 좌측 회전 65.6~73.0°, 그리고 우측 회전 69.4~ 72.0°라고 볼 수 있으며, 이 연구의 사후검사 결과와 상당 부분 일치되는 것으로 보아 이 연구에서 실시한 8주간의 3가지 처치가 앞쪽머리자세 환자의 목뼈 ROM을 정상 범위로 회복시키는데 기여한 것으로 판단된다.
Funk et al.(2003)은 PNF 스트레칭을 실시한 집단에서 통제 집단에 비하여 ROM이 더 크게 향상되었고, 그 효과가 90분 이상 지속되었다고 보고하였다. Kim et al.(2012)은 건강한 20대 성인을 대상으로 근막이완기법을 적용한 결과 목뼈의 폄과 좌·우측 굽힘 ROM이 유의하게 증가되었다고 보고하여 이 연구의 결과와 유사하였다. Saavedra-Hernández et al. (2013)은 만성 목 통증 환자를 대상으로 두 가지 방법의 카이로프랙틱을 1주간 각각 적용한 결과 두 집단 모두에서 목뼈 ROM이 유의하게 개선되었다고 보고하였고, Lee et al.(2014)은 급성 목 통증 환자 8명과 만성 목 통증 환자 8명에게 각각 주 2회, 2주간 카이로프랙틱을 적용한 결과 모든 대상자의 목뼈 ROM이 유의하게 증가되었다고 보고하여 단기간의 처치만으로도 목뼈 ROM의 향상에 도움이 되는 것으로 나타났다.
이 연구에서 카이로프랙틱 집단의 경우 교정을 통하여 목뼈의 정상적인 정렬상태가 확보되어 관절의 해부학적 구조에서 일어나는 기본적인 움직임들이 적절히 나타났기 때문에 ROM의 향상이 가능했던 것으로 사료된다. 또한 목뼈관절 간의 이상적인 정렬상태는 각 척추 분절의 비정상 패턴인 보상적 움직임을 억제하고 선택적 움직임을 촉진하여 정상적인 ROM 회복에 긍정적으로 작용한 것으로 판단된다.
PNF 운동 집단의 경우에는 복합패턴의 효과로 인하여 견갑골의 움직임과 안정성의 증가되고, 몸통 위부분에서 중립자세를 유지하는 능력이 향상되어 목뼈의 앞굽음(lordosis)이 적절하게 형성된 것으로 판단된다. PNF 운동에 따라 나타난 목뼈의 정상적인 정렬상태는 목 부위의 불균형적인 운동부하를 정상적으로 회복시켜 통증의 감소에 긍정적으로 작용하였고, 관절을 구성하는 연부조직의 고유수용기에서 정상적인 신체인식력을 기반으로 새롭게 형성된 신경 지배를 통하여 효율적인 관절의 운동이 가능했던 것으로 사료된다.
한편, 카이로프랙틱+PNF 운동 복합처치 집단에서는 카이로프랙틱 교정을 통하여 뼈대의 정렬상태가 잘 정돈되었고, 이로 인하여 관절에서 이상적인 해부학적 구조가 형성되어 효율적인 근육의 수축이 가능해졌으며, 이와 같은 조건에서 실시한 PNF 운동은 근 기능 회복과 고유수용성 감각의 촉진에 보다 효과적으로 작용하게 되어 정상적인 ROM 회복에 더 큰 영향을 미친 것으로 판단된다.
결 론
이 연구에서는 30명의 앞쪽머리자세 환자를 카이로프랙틱 집단, PNF 운동 집단, 그리고 카이로프랙틱+PNF 운동 복합처치 집단으로 구성하여, 각 집단에서 실시한 처치가 목 부위의 근뼈대계 기능에 미치는 영향을 규명하고자 하였다. 그 결과 세 집단 모두에서 모든 종속변인이 유의하게 변화된 것으로 나타났으며, 카이로프랙틱+PNF 운동 복합처치 집단에서 다른 두 집단에 비하여 그 변화의 양상이 더 뚜렷하게 나타났다. 앞쪽머리전위, 목뼈앞굽음각, 그리고 굽힘과 폄 ROM의 경우 카이로프랙틱+PNF 운동 복합처치 집단에서 다른 두 집단과 비교하여 더 유의한 변화가 나타났다. 좌·우측 굽힘 ROM의 경우 카이로프랙틱+PNF 운동 복합처치 집단에서 PNF 운동 집단에 비해 더 유의한 증가가 나타났다. 이상의 결과를 종합하면, 카이로프랙틱 처치, PNF 운동 처치, 그리고 두 가지의 복합처치 모두 앞쪽머리자세 환자의 근뼈대계 기능 회복에 긍정적으로 작용하였으며, 특히 카이로프랙틱과 PNF 운동을 복합적으로 처치하는 것이 서로의 단점을 보완함으로써 단일 처치에 비하여 더 효과적인 것으로 결론지을 수 있다. 따라서 향후 현장에서는 앞쪽머리자세 환자의 기능 회복을 위하여 카이로프랙틱 처치와 함께 PNF 운동과 같은 능동적 운동을 병행하는 복합처치가 적극적으로 시도되어야 할 것이다.
References
Adler, S. S., Beckers, D., & Buck, M.(2008). PNF in Practice: an Illustrated Guide. 3rd ed., Springer: Berlin, NY.
Adler S. S., Beckers D., et al, Buck M.. 2008. PNF in Practice: an Illustrated Guide 3rd edth ed. Springer. Berlin, NY:Bergmann, T. F. & Peterson, D. H.(2011). Chiropractic Technique: Principles and Procedures. 3rd ed., Elsevier & Mosby: Saint Louis, MO.
Bergmann T. F., et al, Peterson D. H.. 2011. Chiropractic Technique: Principles and Procedures 3rd edth ed. Elsevier & Mosby: Saint Louis, MO.Bonney, R. A. & Corlett, E. N.(2002). Head posture and loading of the cervical spine. Applied Ergonomics, 33(5), 415-417.
Bonney R. A., et al, Corlett E. N.. 2002;Head posture and loading of the cervical spine. Applied Ergonomics 33(5):415–417. 10.1016/s0003-6870(02)00036-4.Brumagne, S., Lysens, R., Swinnen, S., & Verschueren, S.(1999). Effect of paraspinal muscle vibration on position sense of the lumbosacral spine. Spine, 24(13), 1328-1331.
Brumagne S., Lysens R., Swinnen S., et al, Verschueren S.. 1999;Effect of paraspinal muscle vibration on position sense of the lumbosacral spine. Spine 24(13):1328–1331. 10.1097/00007632-199907010-00010.Coulter, I. D., Hurwitz, E. L., Adams, A. H., Genovese, B. J., Hays, R., & Shekelle, P. G.(2002). Patients using chiropractors in North America: who are they, and why are they in chiropractic care? Spine, 27(3), 291-298.
Coulter I. D., Hurwitz E. L., Adams A. H., Genovese B. J., Hays R., et al, Shekelle P. G.. 2002;Patients using chiropractors in North America: who are they, and why are they in chiropractic care? Spine 27(3):291–298.Dishman, J. D., Ball, K. A., & Burke, J.(2002). First prize central motor excitability changes after spinal manipulation: a transcranial magnetic stimulation study. Journal of Manipulative and Physiological Therapeutics, 25(1), 1-9.
Dishman J. D., Ball K. A., et al, Burke J.. 2002;First prize central motor excitability changes after spinal manipulation: a transcranial magnetic stimulation study. Journal of Manipulative and Physiological Therapeutics 25(1):1–9. 10.1067/mmt.2002.120414.Falla, D., Jull, G., Russell, T., Vicenzino, B., & Hodges, P.(2007). Effect of neck exercise on sitting posture in patients with chronic neck pain. Physical Therapy, 87(4), 408-417.
Falla D., Jull G., Russell T., Vicenzino B., et al, Hodges P.. 2007;Effect of neck exercise on sitting posture in patients with chronic neck pain. Physical Therapy 87(4):408–417. 10.2522/ptj.20060009.Funk, D. C., Swank, A. M., Mikla, B. M., Fagen, T. A., & Farr, B. K.(2003). Impact of prior exercise on hamstring flexibility: a comparison of proprioceptive neuromuscular facilitation and static stretching. Journal of Strength and Conditioning Research, 17(3), 489-492
. Funk D. C., Swank A. M., Mikla B. M., Fagen T. A., et al, Farr B. K.. 2003;Impact of prior exercise on hamstring flexibility: a comparison of proprioceptive neuromuscular facilitation and static stretching. Journal of Strength and Conditioning Research 17(3):489–492. 10.1519/1533-4287(2003)017<0489:iopeoh>2.0.co;2.Gabriel, D. A., Kamen, G., & Frost, G.(2006). Neural adaptation to resistive exercise: mechanisms and recommendations for training practices. Sports Medicine, 36(2), 133-149.
Gabriel D. A., Kamen G., et al, Frost G.. 2006;Neural adaptation to resistive exercise: mechanisms and recommendations for training practices. Sports Medicine 36(2):133–149.Gjelsvik, B. E.(2008). The Bobath Concept in Adult Neurology. Thieme: Stuttgart, NY.
Gjelsvik B. E.. 2008. The Bobath Concept in Adult Neurology Thieme: Stuttgart, NY.Gong, W. T., Cheun, H. J., & Lee, K. M.(2010). The effect of cervical stabilized exercise and joint mobilization on maximum muscle strength and static muscle endurance of cervical region. Journal of the Korean data & information science society, 21(1), 33-42.
Gong W. T., Cheun H. J., et al, Lee K. M.. 2010;The effect of cervical stabilized exercise and joint mobilization on maximum muscle strength and static muscle endurance of cervical region. Journal of the Korean data & information science society 21(1):33–42.Häkkinen, A., Salo, P., Tarvainen, U., Wiren, K., & Ylinen, J.(2007). Effect of manual therapy and stretching on neck muscle strength and mobility in chronic neck pain. Journal of Rehabilitation Medicine, 39(7), 575-579.
Häkkinen A., Salo P., Tarvainen U., Wiren K., et al, Ylinen J.. 2007;Effect of manual therapy and stretching on neck muscle strength and mobility in chronic neck pain. Journal of Rehabilitation Medicine 39(7):575–579. 10.2340/16501977-0094.Harrison, D. D., Jackson, B. L., Troyanovich, S., Robertson, G., de George, D., & Barker, W. F.(1994). The efficacy of cervical extension-compression traction combined with diversified manipulation and drop table adjustments in the rehabilitation of cervical lordosis: a pilot study. Journal of Manipulative and Physiological Therapeutics, 17(7), 454-464.
Harrison D. D., Jackson B. L., Troyanovich S., Robertson G., de George D., et al, Barker W. F.. 1994;The efficacy of cervical extension-compression traction combined with diversified manipulation and drop table adjustments in the rehabilitation of cervical lordosis: a pilot study. Journal of Manipulative and Physiological Therapeutics 17(7):454–464.Harrison, D. D., Janik, T. J., Troyanovich, S. J., & Holland, B.(1996). Comparisons oflordotic cervical spine curvatures to a theoretical ideal model of the static sagittal cervical spine. Spine, 21(6), 667-675.
Harrison D. D., Janik T. J., Troyanovich S. J., et al, Holland B.. 1996;Comparisons oflordotic cervical spine curvatures to a theoretical ideal model of the static sagittal cervical spine. Spine 21(6):667–675. 10.1097/00007632-199603150-00002.Harrison, D. E., Harrison, D. D., & Bets J. T.(2003a). Increasing the cervical lordosis with chiropractic biophysics seated combined extension-compression and transverse load cervical traction with cervical manipulation: nonrandomized clinical control trial. Journal of Manipulative and Physiological Therapeutics, 26(3), 139-151.
Harrison D. E., Harrison D. D., Bets J. T.. 2003a;Increasing the cervical lordosis with chiropractic biophysics seated combined extension-compression and transverse load cervical traction with cervical manipulation: nonrandomized clinical control trial. Journal of Manipulative and Physiological Therapeutics 26(3):139–151. 10.1016/s0161-4754(02)54106-3.Harrison, D. E., Harrison D. D., Colloca C. J., Betz, J., Janik, T. J., & Holland, B.(2003b). Repeatability over time of posture, radiograph positioning, and radiograph line drawing: an analysis of six control groups. Journal of Manipulative and Physiological Therapeutics, 26(2), 87-98.
Harrison D. E., Harrison D. D., Colloca C. J., Betz J., Janik T. J., et al, Holland B.. 2003b;Repeatability over time of posture, radiograph positioning, and radiograph line drawing: an analysis of six control groups. Journal of Manipulative and Physiological Therapeutics 26(2):87–98. 10.1067/mmt.2003.15.Health Insurance Review & Assessment Service(2014). Healthcare Bigdata Hub, Health statistical information.
Hoving, J. L., Koes, B. W., de Vet, H. C., van der Windt, D. A., Assendelft, W. J., van Mameren, H., Devillé, W. L., Pool, J. J., Scholten, R. J., & Bouter, L. M.(2002). Manual therapy, physical therapy, or continued care by a general practitioner for patients with neck pain. a randomized controlled trial. Annals of Internal Medicine, 136(10), 713-722.
Hoving J. L., Koes B. W., de Vet H. C., van der Windt D. A., Assendelft W. J., van Mameren H., Devillé W. L., Pool J. J., Scholten R. J., et al, Bouter L. M.. 2002;Manual therapy, physical therapy, or continued care by a general practitioner for patients with neck pain. a randomized controlled trial. Annals of Internal Medicine 136(10):713–722.Huang, Q., Li, D., Zhang, Y., Rui, G., Huo, M., & Maruyama, H.(2014). The intervention effects of different treatments for chronic low back pain as assessed by the thickness of the musculus transversus abdominis. Journal of Physical Therapy Science, 26(9), 1383-1385.
Huang Q., Li D., Zhang Y., Rui G., Huo M., et al, Maruyama H.. 2014;The intervention effects of different treatments for chronic low back pain as assessed by the thickness of the musculus transversus abdominis. Journal of Physical Therapy Science 26(9):1383–1385. 10.1589/jpts.26.1383.Janwantanakul, P., Sitthipornvorakul, E., & Paksaichol, A.(2012). Risk factors for the onset of nonspecific low back pain in office workers: a systematic review of prospective cohort studies. Journal of Manipulative and Physiological Therapeutics, 35(7), 568-577.
Janwantanakul P., Sitthipornvorakul E., et al, Paksaichol A.. 2012;Risk factors for the onset of nonspecific low back pain in office workers: a systematic review of prospective cohort studies. Journal of Manipulative and Physiological Therapeutics 35(7):568–577. 10.1016/j.jmpt.2012.07.008.Jeon, J. K.(2013). The effects of combination patterns exercise of proprioceptive neuromuscular facilitation on balance in chronic low back pain elderly patients. Journal of Digital Convergence, 11(4), 361-368.
Jeon J. K.. 2013;The effects of combination patterns exercise of proprioceptive neuromuscular facilitation on balance in chronic low back pain elderly patients. Journal of Digital Convergence 11(4):361–368.Jull, G.(2000). Deep cervical neck flexor dysfunction in whiplash. Journal of Musculoskeletal Pain, 8(1-2), 143-154.
Jull G.. 2000;Deep cervical neck flexor dysfunction in whiplash. Journal of Musculoskeletal Pain 8(1-2):143–154.Kang, J. H., Park, R. Y., Lee, S. J., Kim, J. Y., Yoon, S. R., & Jung, K. I.(2012). The effect of the forward head posture on postural balance in long time computer based worker. Annals of Rehabilitation Medicine, 36(1), 98-104.
Kang J. H., Park R. Y., Lee S. J., Kim J. Y., Yoon S. R., et al, Jung K. I.. 2012;The effect of the forward head posture on postural balance in long time computer based worker. Annals of Rehabilitation Medicine 36(1):98–104. 10.5535/arm.2012.36.1.98.Kaltenborn, F. M., Evjenth, O., Vollowitz, E., & Kaltenborn, T. B.(2009). Manual Mobilization of the Joints: Joint Examination and Basic Treatment. Volume 2, The Spine. 5th ed., Norli, Oslo.
Kaltenborn F. M., Evjenth O., Vollowitz E., et al, Kaltenborn T. B.. 2009. Manual Mobilization of the Joints: Joint Examination and Basic Treatment 2The Spine. 5th edth ed. Norli. Oslo:Kim, H. N., Yoo, H., Cho, C. M., & Park, G. D.(2011). The Effect of Manual Therapy and Sling Traction Therapy on Cervical Extension Strength and Pain Reduction of Patients with Cervical and Upper Limbs Pain. Korean Journal of Physical Education, 50(2), 355-363.
Kim H. N., Yoo H., Cho C. M., et al, Park G. D.. 2011;The Effect of Manual Therapy and Sling Traction Therapy on Cervical Extension Strength and Pain Reduction of Patients with Cervical and Upper Limbs Pain. Korean Journal of Physical Education 50(2):355–363.Kim, J. C., Jeon, H. S., Yi, C. H., Kwon, O. Y., & Oh, D. W.(2007). Strength and Endurance of the Deep Neck Flexors of Industrial Workers With and Without Neck Pain. Ergonomics Society of Korea, 26(4), 25-31.
Kim J. C., Jeon H. S., Yi C. H., Kwon O. Y., et al, Oh D. W.. 2007;Strength and Endurance of the Deep Neck Flexors of Industrial Workers With and Without Neck Pain. Ergonomics Society of Korea 26(4):25–31. 10.5143/jesk.2007.26.4.025.Kim, J. S., & Kim, T. W.(2008). Effect of manual remedy therapy on patients with cervical hypolordosis. Korean Journal of Physical Education, 47(2), 391-400.
Kim J. S., et al, Kim T. W.. 2008;Effect of manual remedy therapy on patients with cervical hypolordosis. Korean Journal of Physical Education 47(2):391–400.Kim, J. S., Moon, D. C., & Chang, K. S.(2012). Changes of Flexibility and Plasma Catecholamine by Myofascial Release Approach. The Korea Contents Society, 12(3), 214-221.
Kim J. S., Moon D. C., et al, Chang K. S.. 2012;Changes of Flexibility and Plasma Catecholamine by Myofascial Release Approach. The Korea Contents Society 12(3):214–221. 10.5392/jkca.2012.12.03.214.Kim, Y. H., & Khil, J. H.(2010). Effects of Chiropractic Treatment and Low Back Exercise on Flexibility, Cervical Lordosis Angle, and Pelvic Deviation in Low Back Pain Patients. Korean Association of Certified Exercise Professionals, 12(3), 97-106.
Kim Y. H., et al, Khil J. H.. 2010;Effects of Chiropractic Treatment and Low Back Exercise on Flexibility, Cervical Lordosis Angle, and Pelvic Deviation in Low Back Pain Patients. Korean Association of Certified Exercise Professionals 12(3):97–106.Kofotolis, N. & Kellis, E.(2006). Effects of two 4-week proprioceptive neuromuscular facilitation programs on muscle endurance, flexibility, and functional performance in women with chronic low back pain. Physical Therapy, 86(7), 1001-1012.
Kofotolis N., et al, Kellis E.. 2006;Effects of two 4-week proprioceptive neuromuscular facilitation programs on muscle endurance, flexibility, and functional performance in women with chronic low back pain. Physical Therapy 86(7):1001–1012.Korr, I. M.(1995). Proprioceptors and somatic dysfunction. The Journal of the American Osteopathic Association, 74(7), 638-650.
Korr I. M.. 1995;Proprioceptors and somatic dysfunction. The Journal of the American Osteopathic Association 74(7):638–650.Kwon, W. A., Kim, D. D., & Lee, J. H.(2010). The Effects of Massage and Static Stretching on Cervical Range of Motion in Their 20s of Normal Adult. Journal of the Korea Academia-Industrial Cooperation Society, 11(11), 4346-4353.
Kwon W. A., Kim D. D., et al, Lee J. H.. 2010;The Effects of Massage and Static Stretching on Cervical Range of Motion in Their 20s of Normal Adult. Journal of the Korea Academia-Industrial Cooperation Society 11(11):4346–4353. 10.5762/kais.2010.11.11.4346.Lantz, C. A., Chen, J., & Buch, D.(1999). Clinical validity and stability of active and passive cervical range of motion with regard to total and unilateral uniplanar motion. Spine, 24(11), 1082-1089.
Lantz C. A., Chen J., et al, Buch D.. 1999;Clinical validity and stability of active and passive cervical range of motion with regard to total and unilateral uniplanar motion. Spine 24(11):1082–1089. 10.1097/00007632-199906010-00007.Lee, C. W., Hwangbo, K., & Lee, I. S.(2014). The effects of combination patterns of proprioceptive neuromuscular facilitation and ball exercise on pain and muscle activity of chronic low back pain patients. Journal of Physical Therapy Science, 26(1), 93-96.
Lee C. W., Hwangbo K., et al, Lee I. S.. 2014;The effects of combination patterns of proprioceptive neuromuscular facilitation and ball exercise on pain and muscle activity of chronic low back pain patients. Journal of Physical Therapy Science 26(1):93–96. 10.1589/jpts.26.93.Lee, J. R., Oh, C. U., Lee, M. S., & Suh, D. W.(2014). The Influences of Chiropractic Therapy on Neck Pain Patients. Journal of the Korea Academia-Industrial Cooperation Society, 15(3), 1496-1505.
Lee J. R., Oh C. U., Lee M. S., et al, Suh D. W.. 2014;The Influences of Chiropractic Therapy on Neck Pain Patients. Journal of the Korea Academia-Industrial Cooperation Society 15(3):1496–1505. 10.5762/kais.2014.15.3.1496.Lohman, T. G., Roche, A. F., & Martorell, R.(1992). Anthropometric Standardization Reference Manual. Human Kinetics: Champaign, IL.
Lohman T. G., Roche A. F., et al, Martorell R.. 1992. Anthropometric Standardization Reference Manual Human Kinetics: Champaign, IL. 10.1249/00005768-199208000-00020.Morningstar, M. W.(2006). Improvement of lower extremity electrodiagnostic findings following a trial of spinal manipulation and motion-based therapy. Chiropractic and Osteopathy, 12, 14-20.
Morningstar M. W.. 2006;Improvement of lower extremity electrodiagnostic findings following a trial of spinal manipulation and motion-based therapy. Chiropractic and Osteopathy 12:14–20.Norkin, C. C. & White, D. J.(2009). Measurement of Joint Motion: a Guide to Goniometry. 4th ed., F. A. Davis Company: Philadelphia, PA.
Norkin C. C., et al, White D. J.. 2009. Measurement of Joint Motion: a Guide to Goniometry 4th edth ed. F. A. Davis Company: Philadelphia, PA.Ogura, T., Tashiro, M., Masud, M., Watanuki, S., Shibuya, K., Yamaguchi, K., Itoh, M., Fukuda, H., & Yanai, K.(2011). Cerebral metabolic changes in men after chiropractic spinal manipulation for neck pain. Alternative Therapies in Health and Medicine, 17(6), 12-17.
Ogura T., Tashiro M., Masud M., Watanuki S., Shibuya K., Yamaguchi K., Itoh M., Fukuda H., et al, Yanai K.. 2011;Cerebral metabolic changes in men after chiropractic spinal manipulation for neck pain. Alternative Therapies in Health and Medicine 17(6):12–17.Oh, D. G., Sung, S. C., & Lee, M. G.(2011). Effects of elastic band exercise using PNF and CNS-stimulating exercise on functional fitness and EMG in hemiplegic stroke patients. The Korean Society of Sports Science, 20(2), 815-827.
Oh D. G., Sung S. C., et al, Lee M. G.. 2011;Effects of elastic band exercise using PNF and CNS-stimulating exercise on functional fitness and EMG in hemiplegic stroke patients. The Korean Society of Sports Science 20(2):815–827.Oh, H. J., Hwang, B. J., & Choi Y. R.(2014). Effects of Cervical Joint Mobilization on the Forward Head Posture and Neck Disability Indexes. The Korean Society of Radiology. 8(2), 89-96.
Oh H. J., Hwang B. J., Choi Y. R.. 2014;Effects of Cervical Joint Mobilization on the Forward Head Posture and Neck Disability Indexes. The Korean Society of Radiology 8(2):89–96. 10.7742/jksr.2014.8.2.89.Oh, W. K., Lee, E. G., & Shin, B. C.(2009). Clinical Effect of Bong Chuna Manual Therapy and Acupunture Treatment for Improving Cervical Curvature of Turtle Neck Syndrome and Measurement Method of Radiography. Journal of Oriental Rehabilitation Medicine, 19(1), 113-124.
Oh W. K., Lee E. G., et al, Shin B. C.. 2009;Clinical Effect of Bong Chuna Manual Therapy and Acupunture Treatment for Improving Cervical Curvature of Turtle Neck Syndrome and Measurement Method of Radiography. Journal of Oriental Rehabilitation Medicine 19(1):113–124.O’Leary, S., Falla, D., Jull, G., & Vicenzino, B.(2007). Muscle specificity in tests of cervical flexor muscle performance. Journal of Electromyography and Kinesiology, 17(1), 35-40.
O’Leary S., Falla D., Jull G., et al, Vicenzino B.. 2007;Muscle specificity in tests of cervical flexor muscle performance. Journal of Electromyography and Kinesiology 17(1):35–40. 10.1016/j.jelekin.2005.10.006.Olson, S. L., O'Connor, D. P., Birmingham, G., Broman, P., & Herrera, L.(2000). Tender point sensitivity, range of motion, and perceived disability in subjects with neck pain. Journal of Orthopaedic and Sports Physical Therapy, 30(1), 13-20.
Olson S. L., O'Connor D. P., Birmingham G., Broman P., et al, Herrera L.. 2000;Tender point sensitivity, range of motion, and perceived disability in subjects with neck pain. Journal of Orthopaedic and Sports Physical Therapy 30(1):13–20. 10.2519/jospt.2000.30.1.13.Pearson, N. D. & Walmsley, R. P.(1995). Trial into the effects of repeated neck retractions in normal subjects. Spine, 20(11), 1245-1250.
Pearson N. D., et al, Walmsley R. P.. 1995;Trial into the effects of repeated neck retractions in normal subjects. Spine 20(11):1245–1250. 10.1097/00007632-199506000-00006.Que, Q., Ye, X., Su, Q., Weng, Y., Chu, J., Mei, L., Huang. W., Lu. R., & Zheng. G.(2013). Effectiveness of acupuncture intervention for neck pain caused by cervical spondylosis: study protocol for a randomized controlled trial. Trials, 14, 186-192.
Que Q., Ye X., Su Q., Weng Y., Chu J., Mei L., Huang W., Lu R., Zheng G.. 2013;Effectiveness of acupuncture intervention for neck pain caused by cervical spondylosis: study protocol for a randomized controlled trial. Trials 14:186–192. 10.1186/1745-6215-14-186.Ribeiro, T., Britto, H., Oliveira, D., Silva, E., Galvão, E., & Lindquist, A.(2013). Effects of treadmill training with partial body weight support and the proprioceptive neuromuscular facilitation method on hemiparetic gait: a randomized controlled study. European Journal of Physical and Rehabilitation Medicine, 49(4), 451-461.
Ribeiro T., Britto H., Oliveira D., Silva E., Galvão E., et al, Lindquist A.. 2013;Effects of treadmill training with partial body weight support and the proprioceptive neuromuscular facilitation method on hemiparetic gait: a randomized controlled study. European Journal of Physical and Rehabilitation Medicine 49(4):451–461.Rubini, E. C., Souza, A. C., Mello, M. L., Bacurau, R. F., Cabral, L. F., & Farinatti, P. T.(2011). Immediate effect of static and proprioceptive neuromuscular facilitation stretching on hip adductor flexibility in female ballet dancers. Journal of Dance Medicine and Science, 15(4), 177-181.
Rubini E. C., Souza A. C., Mello M. L., Bacurau R. F., Cabral L. F., et al, Farinatti P. T.. 2011;Immediate effect of static and proprioceptive neuromuscular facilitation stretching on hip adductor flexibility in female ballet dancers. Journal of Dance Medicine and Science 15(4):177–181.Saavedra-Hernández, M., Arroyo-Morales, M., Cantarero-Villanueva, I., Fernández-Lao, C., Castro-Sánchez, A. M., Puentedura, E. J., & Fernández-de-las-Peñas, C.(2013). Short-term effects of spinal thrust joint manipulation in patients with chronic neck pain: a randomized clinical trial. Clinical Rehabilitation, 27(6), 504-512.
Saavedra-Hernández M., Arroyo-Morales M., Cantarero- Villanueva I., Fernández-Lao C., Castro-Sánchez A. M., Puentedura E. J., et al, Fernández-de-las-Peñas C.. 2013;Short-term effects of spinal thrust joint manipulation in patients with chronic neck pain: a randomized clinical trial. Clinical Rehabilitation 27(6):504–512. 10.1177/0269215512464501.Shin, D. C., Shin, W. S., & Song C. H.(2008). The Effects of a Deep Cervical Flexion Exercise for Sedentary Workers with VDT Syndrome. Ergonomics Society of Korea, 27(4), 59-64.
Shin D. C., Shin W. S., Song C. H.. 2008;The Effects of a Deep Cervical Flexion Exercise for Sedentary Workers with VDT Syndrome. Ergonomics Society of Korea 27(4):59–64.Ylinen, J., Salo, P., Nykänen, M., Kautiainen, H., & Häkkinen, A.(2004). Decreased isometric neck strength in women with chronic neck pain and the repeatability of neck strength measurements. Archives of Physical Medicine and Rehabilitation, 85(8), 1303-1308.
Ylinen J., Salo P., Nykänen M., Kautiainen H., et al, Häkkinen A.. 2004;Decreased isometric neck strength in women with chronic neck pain and the repeatability of neck strength measurements. Archives of Physical Medicine and Rehabilitation 85(8):1303–1308.Yochum, T. R. & Rowe, L. J.(2005). Essentials of Skeletal Radiology. 3rd ed., Lippincott Williams & Wilkins: Philadelphia, PA.
Yochum T. R., et al, Rowe L. J.. 2005. Essentials of Skeletal Radiology 3rd edth ed. Lippincott Williams & Wilkins: Philadelphia, PA.Yoo, W. G.(2013). Effect of thoracic stretching, thoracic extension exercise and exercises for cervical and scapular posture on thoracic kyphosis angle and upper thoracic pain. Journal of Physical Therapy Science, 25(11), 1509-1510.
Yoo W. G.. 2013;Effect of thoracic stretching, thoracic extension exercise and exercises for cervical and scapular posture on thoracic kyphosis angle and upper thoracic pain. Journal of Physical Therapy Science 25(11):1509–1510. 10.1589/jpts.25.1509.Youdas, J. W., Garrett, T. R., Suman, V. J., Bogard, C. L., Hallman, H. O., & Carey, J. R.(1992). Normal range of motion of the cervical spine: an initial goniometric study. Physical Therapy, 72(11), 770-780.
Youdas J. W., Garrett T. R., Suman V. J., Bogard C. L., Hallman H. O., Carey J. R.. 1992;Normal range of motion of the cervical spine: an initial goniometric study. Physical Therapy 72(11):770–780. 10.1093/ptj/72.11.770.