걷기 운동 시 심박수와 가속도센서를 이용한 VO2max 간접측정법 개발
Estimation of VO2max from walk exercises with heart rate and accelerometer
Article information
Abstract
목적
본 연구는 20대 남녀를 대상으로 일정속도로 걷기 시 심박수와 가속도센서를 이용하여 신뢰도와 타당도, 경제성이 높은 VO2max간접측정법을 개발하였다.
방법
총 107명(남성: 55명, 여성: 52명)의 연구대상자는 신체구성 측정 후 운동부하테스트와 두 번의 1,600 m 걷기(빠르게 걷기, 일정속도 걷기)에 참여하였다. 연구대상자의 연령과 신체적 특성, 그리고 걷기 시 측정된 시간, heart rate (HR), 또는 HR과 activity count per minute (ACM)의 비율(HR/ACM)을 변인으로 회귀분석을 시행하였다. 개발된 추정식의 타당도 검증을 위하여 직접법에 의한 VO2max와 추정식에 의한 VO2max의 상관관계분석과 예측잔차합제곱(predicted residual sum of squares)를 시행하였다. 또한, 직접법에 의한 VO2max와 추정식에 의한 VO2max의 차이를 분석하기 위하여 Bland-Altman plotting과 선형회귀분석을 실시하였다.
결과
구간별(400 m, 800 m, 1,200 m, 1,600 m) HR/ACM과 걷기시간이 성별, 연령과 함께 직접법에 의한 VO2max와 유의한 상관관계가 나타났다. 모든 구간에서 추정식이 개발되었으나 400m에서만 직접법에 의한 VO2max와 차이가 없었다(R2: 0.675, %SEE: 10.7). VO2max=121.659+6.656×Gender-0.865×Age-9.540×Time-2460.952×HR/ACM (Gender, 0= female, 1=male: Time, hundredth of a minute: HR, heart rate: ACM, activity count per minute). 모든 구간에서 빠르게 걷기보다 일정속도로 걷기 시 운동강도(%HRmax)가 낮게 나타났다.
결론
따라서 본 연구를 통해 개발된 추정식을 통해 보다 짧은 거리 또는 보다 낮은 강도의 걷기를 통해 20대 성인의 VO2max측정이 가능할 것으로 사료된다.
Trans Abstract
Purpose
The purpose of this study was to develop the new indirect method assessing maximal oxygen uptake (VO2max) using heart rate (HR) and accelerometer during walk exercise.
Methods
One hundred seven participants (55 male, 52 female) performed a graded exercise test to determine VO2max and two types of 1,600 m walk exercises (fast walk and pace controlled walk). The equations for estimating VO2max was developed by stepwise multiple regression. The validity of developed equations tested through the correlation between measured VO2max and estimated VO2max, was assessed by predicted residual sum of squares, and Bland-Altman plotting.
Results
VO2maxwas correlated with time, and HR/activity count per minute (ACM) measured in pace controlled walk exercise at all distance (400 m, 800 m, 1,200 m, 1,600 m). The equations were valid significantly and their multiple correlation coefficients or standard estimated error were similar to that Åstrand-Rhyming cycle ergometer test or Rockport 1 mile walk test. Using HR/ACM in pace controlled walk (400 m), it was possible to estimate VO2max(R2: 0.675, %SEE: 10.7). The equation was: VO2max=121.659+6.656×Gender-0.865×Age-9.540×Time-2460.952×HR/ACM (Gender, 0=female, 1=male: Time, hundredth of a minute: HR, heart rate: ACM, activity count per minute).
Conclusion
Estimation equations developed in this study are considered to estimate VO2max through a shorter distance, or a lower intensity of walk exercise. It is required studies to target a wide range of ages or to develop walk test on a lower bpm.
서론
심폐지구력은 일반인의 건강과 가장 밀접한 관련이 있는 체력 요소이다(American College of Sports Medicine, 2010). 심폐지구력의 저하는 심혈관계 질환의 사망률과 이환율의 증가와 관련이 있으며(Wei et al., 1999; Katzmarzyk et al., 2004), 이러한 결과는 질환자뿐만 아니라 건강인의 사망률도 증가시킨다(Kodama et al., 2009). 심폐지구력의 평가는 운동강도를 결정하는 중요한 요소 일뿐만 아니라 개인의 건강상태를 평가함에 있어 유용한 지표가 된다(ACSM, 2010). 심폐지구력은 최대산소섭취량(maximal oxygen uptake: VO2max)으로 평가된다. VO2max는 트레드밀이나 고정식 자전거에르고미터를 이용하여 대상자가 호흡하는 환기량 및 산소와 이산화탄소 농도를 측정하는 최대 운동부하테스트, 또는 탈진상태(all out)에 이르지 않아도 되는 최대하 운동부하테스트 및 필드테스트를 통해 타당도를 추정할 수 있다(Powers & Howley, 2008; Westerterp & Bouten, 1997; Cao et al., 2010).
최대 또는 최대하 운동부하테스트는 대상자의 높은 운동수준이 요구되거나 개인의 동기수준이나 운동능력 등이 측정에 영향을 줄 수 있다. 또한, 고가의 장비와 공간, 그리고 전문인력이 필요하여 실용적인 측면에서 다소 제한적이다(Weyand et al., 2001; Plasqui & Westerterp, 2006). 이에 비해 필드테스트는 특정 거리를 걷거나 달리는데 걸리는 시간이나 특정 시간에 걷거나 달린 거리 등을 측정하여 VO2max을 추정하는 방법으로 한 번에 여러 사람을 동시에 측정할 수 있고 초시계와 같은 최소한의 장비만 있으면 가능하다(Kline et al., 1987; ACSM, 2010). 그러나 여전히 대상자가 높은 수준의 신체적인 능력을 발휘하여야 한다. 이 경우 운동 시 개인의 동기수준과 조절능력이 영향을 미칠 수 있다. 또한, 필드테스트의 주요 측정변인인 심박수(heart rate: HR)는 유전, 연령, 운동습관의 유무 등에 영향을 받으며 약물의 복용과 질환의 유무 등에 따라 쉽게 변하며 운동부하가 불규칙하거나 HR이 항정상태가 되지 않은 경우에 오차가 발생할 수 있다(Luke et al., 1997; Achten & Jeukendrup, 2003; Plasqui & Westerterp, 2005). 따라서 Rockport 1마일 걷기테스트를 최대 능력으로 걷기가 아니라 bpm(beat per minute)과 같은 객관적인 기준으로 일정한 페이스로 걷기를 시행하면 일반인이 시행하기 용이하면서 항정상태의 HR을 측정할 수 있으므로 최대하 운동부하테스트처럼 운동강도에 대한 HR을 적용시킬 수 있어 VO2max에 대한 신뢰도와 타당도 높게 추정할 수 있을 것으로 사료된다.
최근 지면반력시간을 이용하여 트레드밀에서 달리기를 통해 측정된 운동강도에 대한 HR을 이용하여 VO2max를 추정하는 방법을 제안하였다(Weyand et al., 2001). 그러나 이 방법은 트레드밀에서 최소 2 m/sec의 속도로 달리기를 시행하여야 하며 실제 필드에서 검증이 이뤄지지 않았을 뿐만 아니라, 지면반력시간을 측정할 수 있는 electronic foot contact monitor의 개발도 더 이상 이뤄지지 않았다. 최근 개발되고 있는 가속도계를 이용하여 운동강도를 측정할 수 있다. 가속도계는 크기가 작아 다양한 상황에서 신체활동을 측정할 수 있는 타당도 높은 장비(Kumahara et al., 2004; Kavanagh & Menz, 2008)로 활동량(amount), 빈도(frequency), 강도(intensity)등의 다양한 활동정보를 제공해준다(Butte et al., 2012). 가속도계는 activity count를 측정하여 신체활동량과 강도 등을 평가 할 수 있다(Treuth et al., 2004). 신체활동량은 하루 동안의 activity count의 합으로 나타낼 수 있으며, 활동 강도는 분당 activity count의 합(activity count per minute: ACM)으로 나타낼 수 있다. 분당 activity count의 합이 클수록 활동강도가 크다고 할 수 있다(Plasqui & Westerterp, 2005). 최근에는 3축(vertical, medial-lateral, anterior-posterior) 가속도계의 개발로 저강도 뿐만 아니라 빨리 걷기나 달리기와 같은 고강도 운동 시에도 ACM을 이용하여 신체활동량의 측정이 가능하게 되었다(Westerterp & Bouten, 1997; Fudge et al., 2007; Rowlands et al., 2007). 따라서 3축의 가속도계와 심박계를 이용하면 다양한 운동 시 운동강도에 대한 HR을 구할 수 있을 것이다. 이에 Plasqui & Westerterp (2005)는 7일 동안 일상생활의 HR과 ACM을 측정하여 HR과 ACM의 비율(HR/ACM)을 산출하고 이를 체력지수(fitness index)라고 명하였다. 이 체력지수는 VO2max와 유의한 상관을 나타내 일상생활의 HR과 ACM 만으로 VO2max을 측정할 수 있으나 7일 동안 연속해서 측정해야 하고 가속도계로 정적활동 시 신체활동량을 정확하게 측정할 수 없다는 제한점이 있다. 그러나 이 체력지수를 단시간 동안 동적활동을 수행하는 필드테스트에 도입한다면 기존의 필드테스트보다 신뢰도와 타당도 높게 VO2max를 추정할 수 있을 것으로 사료된다.
따라서 본 연구는 심박수와 가속도계를 이용하여 일반인이 시행하기에 용이하고, 신뢰도와 타당도 높게 VO2max를 추정할 수 있는 필드테스트를 개발하고자 하였다.
연구방법
연구설계와 절차
본 연구는 107명의 20대 남녀를 대상으로 시행하였다. 일반적으로 추정식 개발에 필요한 연구대상자 수는 변인 당 15~30명 또는 통계적 분석을 통해 결정하여야 한다(Palmer & OʼConnell, 2009). 본 연구에서는 G power 프로그램을 이용하여 신뢰도와 타당도 높은 추정식 개발을 위해 유의수준(α) 5%, 검정력(β) 80%, 효과크기 0.15 조건으로 필요한 대상자 수를 산출하였다(Faul et al., 2007). 걷기 활동은 체력 수준에 상관없이 누구나 참여할 수 있는 신체활동으로 본 연구는 Rockport 1마일 걷기와 이의 변형 걷기를 시행하였다. 따라서 본 연구에 참여한 모든 연구대상자는 신체구성 측정 후 한 번의 운동부하테스트와 두 가지의 서로 다른 형태의 걷기(빠르게 걷기, 일정속도 걷기)에 참여하였다. 대상자의 최대능력을 유도하기 위하여 각 테스트 간에 48시간 동안 휴식을 취하게 하였다.
연구대상자
본 연구는 광고를 통해 모집된 20대 참여자 총 108명(남성 55명, 여성 53명)을 대상으로 하였다. 이 중 VO2max측정이 불가능했던 1명(사유: 측정중지 요청)을 제외한 107명(남성: 55명, 여성: 52명)을 대상으로 측정 결과를 분석하였다. 측정 전에 건강설문조사를 시행하여 근골격계 질환이나 만성질환이 있는 경우와 HR이나 혈압에 영향을 줄 수 있는 약을 복용하는 경우에는 연구대상자에서 제외하였다. 연구 참가에 앞서 모든 연구대상자들에게 연구의 내용과 목적을 자세히 설명한 후 연구 참가동의서에 서명을 받은 후 참여토록 하였다. 본 연구대상자의 신체적 특성은 <Table 1>과 같다. 대상자의 직접법에 의한 VO2max의 범위는 27.2~63.5 ml/kg/min (여성은 27.2~52.4 ml/kg/min, 남성은 36~63.5 ml/kg/min)으로 체력수준이 다양하였으며, 전체 대상자의 45.8%(여성: 42.3%, 남성: 49.1%)가 주 3 회, 1 회 30 분 이상, 중강도 운동을 시행하는 운동습관이 있는 집단으로 나타났다.

Characteristics of subjects
(Mean±STD)
측정내용 및 방법
신체계측 및 혈압측정
신체구성은 생체전기저항법(X-Scan Plus Ⅱ, Korea)을 이용하여 신장(height), 체중(weight), 체지방량(fat mass), 체지방율(%body fat)을 측정하였다. 대상자가 가벼운 복장을 한 상태에서 성별 및 연령을 입력하고 양손으로 손잡이를 잡고 팔을 약간 벌리고 똑바로 선 자세로 측정하였다. 신체질량지수(body mass index: BMI)는 체중과 신장의 제곱 비율(kg/㎡)로 산출하였다.
운동부하테스트
대상자가 실험실에 도착한 후 안정을 취하게 하여 안정 시 HR과 혈압을 확인한 후, 트레드밀(Marquett Series 2000, USA)과 자동호흡가스분석기(Ultima CPX, USA)를 사용하여 운동부하테스트를 실시하였다. 운동부하 방법은 속도는 1.7 mph, 경사도는 0%로 운동을 시작하여, 매 단계마다 측정중지 시까지 속도(0.89 mph) 또는 경사도(5%)를 증가시켰다(modified Bruce protocol)(Bruce & McDonough, 1969; Grossman et al., 1990).
운동부하 중에는 운동자각도(rating of perceived exertion: RPE)로 대상자의 주관적 운동강도를 파악하였으며(Borg, 1973), 본인이 의지적으로 더 이상 운동을 더 이상 할 수 없는 all-out 상태에 도달하였을 때 또는 속도를 따라가지 못할 때, 이상 증상 발현 시에 즉각 정지될 수 있도록 하여 운동 중 불의의 사고를 예방하였다. 테스트 종료 후 정리운동을 시행하였으며 그 후 의자에 앉아 최대한 편안한 상태에서 5분간 휴식을 취하도록 하였다.
VO2max의 판정조건은 1)운동강도가 증가하여도 VO2가 더 이상 증가하지 않을 때(leveling off), 2)호흡교환율(respiratory exchange ratio: RER)이 1.15이상일 때, 3)대상자의 HR이 최대예측 HR의 90% 이상일 때, 4)RPE가 18이상일 때, 5)대상자가 중지 의사를 표현할 때의 다섯 가지 중 세 가지 이상 만족시키는 것으로 하였다(Howley et al., 1995; Evans et al., 2013).
빠르게 걷기
빠르게 걷기는 Rockport 1마일 걷기테스트와 동일한 방법으로 진행하였다(Kline et al., 1987). 측정을 시작하기 전에 대상자들에게 충분히 방법을 설명한 후 테스트 시작 직전에 안정 시 HR을 확인하고 측정을 시작하였다. 대상자로 하여금 뛰거나 멈추지 말고 가능한 빠르게 1,600 m를 걷도록 하였으며, 400 m, 800 m, 1,200 m, 그리고 1,600 m 구간마다 시간, HR, 그리고 ACM을 측정하였다.
일정속도 걷기
일정속도 걷기는 Rockport 1마일 걷기를 변형하여 진행하였다. 대상자로 하여금 뛰거나 멈추지 말고 140 bpm에 맞춰진 메트로놈의 소리에 맞추어 1,600 m를 걷도록 하였으며, 400 m, 800 m, 1,200 m, 그리고 1,600 m 구간마다 시간, HR, 그리고 ACM을 측정하였다.
HR과 ACM 측정
Transmitter belt가 부착된 심박계(Polar RS 400 TM, Finland)를 가슴에 착용하여 도착시 HR를 측정하였다. ACM의 측정을 위해서 작고(33.5×12.5×33.5 mm) 가벼워(약 13.2 g) 운동 시 방해가 되지 않는 3축 가속도계(Life gram LA 11 M-BS, Korea)를 허리에 착용하여 측정하였다(Choi et al., 2011). Life gram은 ±8 g의 가속도 범위를 측정할 수 있으며 표본화 주파수(sampling frequency)가 20Hz로 설정된 장비로 일상생활 활동뿐만 아니라 걷기와 달리기 시에도 ACM을 측정할 수 있다. AMC은 활동량계로 측정되는 기본 단위이며 보수, 활동 빈도, 에너지 소모량 등은 ACM을 변환하여 산출되게 된다.
걷기 운동 시 activity count는 3축(vertical, x; medial-lateral, y; anterior-posterior, z)의 각 벡터제곱의 합의제곱근(
자료처리
본 연구에서 측정된 모든 항목의 결과는 기술통계분석을 이용하여 평균과 표준편차로 표기하였다. 모든 분석은 SPSS for Windows (version 21.0) 통계 프로그램을 이용하였다. 모든 통계치의 유의수준(α)은 .05로 하였다.
추정식 개발
빠르게 걷기와 일정속도 걷기의 운동 강도 차이를 비교하기 위하여 구간별 %HRmax를 대응표본 t 검증으로 비교하였다. 직접법에 의한 VO2max와 연령 및 신장, 체중 등 대상자 특성 그리고 빠르게 걷기 또는 일정속도 걷기 시의 구간별(400 m, 800 m, 1,200 m, 1,600 m) 걷기시간, HR 또는 HR/ACM의 상관관계 검증을 위하여 피어슨 상관관계분석(Pearsonʼs product correlation)을 실시하여 상관계수(r)를 산출하였다. VO2max를 예측하기 위한 추정식 개발을 위하여 회귀분석(regression analysis)을 실시하였다. 회귀분석 시 종속변수와 가장 높은 편상관관계를 갖는 변수를 선택하고 비유의적인 변수는 제거하기 위하여 단계선택(stepwise)방법으로 시행하였다. 단계적 회귀분석 시 추정식의 적합도는 다중상관계수(R), 수정된 상관계수 제곱(adjR2), 표준추정오차(Standard Error of Estimate, SEE), 표준추정 오차비율(percentage of SEE, %SEE) (SEE/VO2max평균 ×100), Mallow’s Cp (Cp)로 평가하였다(Palmer & OʼConnell, 2009).
타당도 검증
직접법에 의한 VO2max와 추정식에 의한 VO2max의 상관관계 검증을 위하여 피어슨 상관관계분석(Pearson’s product correlation)을 실시하여 상관계수(r)를 산출하였다. 추정식의 교차타당도 검증을 위해 예측 잔차합 제곱(predicted residual sum of squares: PRESS) 분석을 통해 직접법에 의한 VO2max와 추정식에 의한VO2max간의 PRESS 다중상관계수(Rp)와 PRESS SEE (SEEp)를 산출하였다(Holiday et al., 1995; George et al., 1997; Palmer & OʼConnell, 2009). 직접법에 의한 VO2max와 추정식에 의한 VO2max간 차이가 나는지 분석하기 위하여 Bland-Altman plotting과 선형회귀분석(linear regression analysis)을 실시하였다(Bland & Altman, 1986).
연구결과
VO2max와 신체적 특성의 상관관계.
직접법에 의한 VO2max와 신체적 특성의 상관관계를 분석한 결과 연령과 체지방율이 증가할수록 VO2max는 감소하고 신장 및 체중이 증가할수록 직접법에 의한 VO2max는 증가하였다(p<0.01). 따라서 VO2max추정식 개발을 위한 회귀분석 시 연령과 체중을 독립변인으로 사용하였다<Table 2>.

Correlation between VO2max and subjectsʼ characteristics
VO2max와 걷기시간, 심박수, HR/ACM의 상관관계
일정속도로 걷기 동안 측정한 구간별 시간 또는 HR과 직접법에 의한 VO2max의 상관관계 분석결과 시간과 HR이 증가할수록 VO2max가 감소하였다(p<0.01). 또한 일정속도로 걷기 동안 측정한 구간별 상관관계는 HR/ACM이 증가할수록 VO2max가 감소하였다(p<0.001)<Table 3>.

Correlation between VO2max and pace controlled walkʼs variables
일정속도로 걷기 시 HR/ACM을 이용한 VO2max추정식
일정속도로 걷기 시 모든 구간에서 측정한 HR/ACM을 독립변수로 하여 회귀분석 결과, 체중을 제외한 성별, 연령, 시간, HR/ACM이 VO2max와 유의한 상관이 있었다(p<0.001)<Table 4>. 각 구간별 다중상관계수(R)가 각각 0.822 (400 m), 0.832 (800 m), 0.841 (1,200 m), 0.835 (1,600 m)으로 VO2max변동량(R2)의 67.6% (400 m), 69.2% (800 m), 70.7% (1,200 m), 69.7% (1,600 m)를 각각 설명할 수 있다<Table 4>. 교차검증분석을 위한 PRESS 분석결과 각 구간의 다중상관계수(Rp)와 SEEp는 회귀분석의 다중상관계수와 SEE에 비하여 변화폭이 낮았다<Table 4>. 직접법에 의한 VO2max와 추정식에 의한 VO2max의 상관관계는 상관계수가 각각 0.816 (400 m), 0.825 (800 m), 0.825 (1,200 m), 0.820 (1,600 m)으로 유의하게 나타났다(p<0.001)<Fig. 1>. 하지만, 직접법에 의한 VO2max가 57.5 ml/kg/min 이상인 경우 과소추정 되는 경향으로 VO2max가 57.5 ml/kg/min 이상인 경우를 제외하고 Bland-Altman plotting 분석을 시행하였다. 그 결과 직접법에 의한 VO2max와 400 m 일정속도로 걷기(HR/ACM 400 m) 또는 800 m 일정속도로 걷기 (HR/ACM 800 m), 1,200 m 일정속도로 걷기(HR/ACM 1,200 m), 1,600 m 일정속도로 걷기(HR/ACM 1,600 m) 추정식에 의한 VO2max간에 통계적으로 차이가 나타나지 않았다<Fig. 2>.

Multiple regression models with VO2max and HR/ACM from pace controlled walk
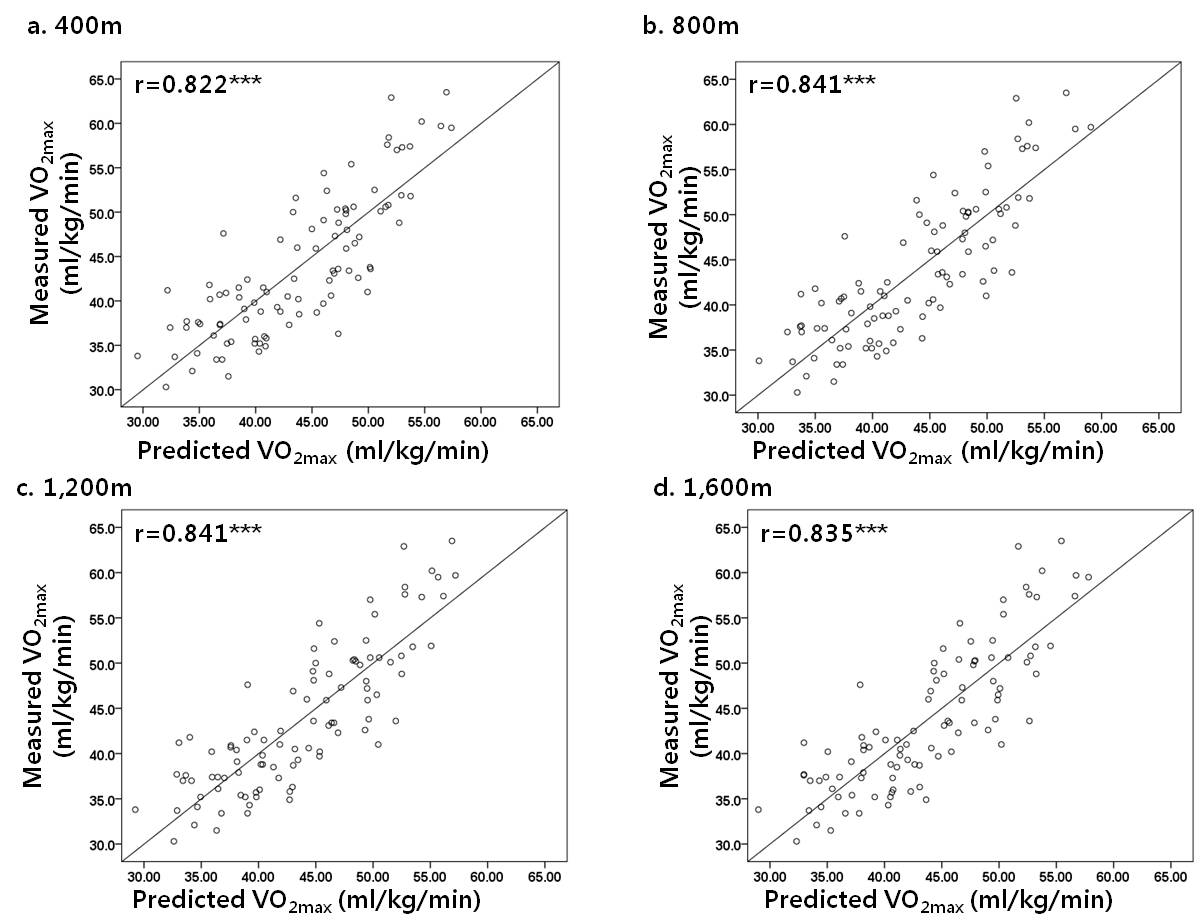
Correlation between the measured and predicted VO2max with HR/ACM from pace controlled walk.
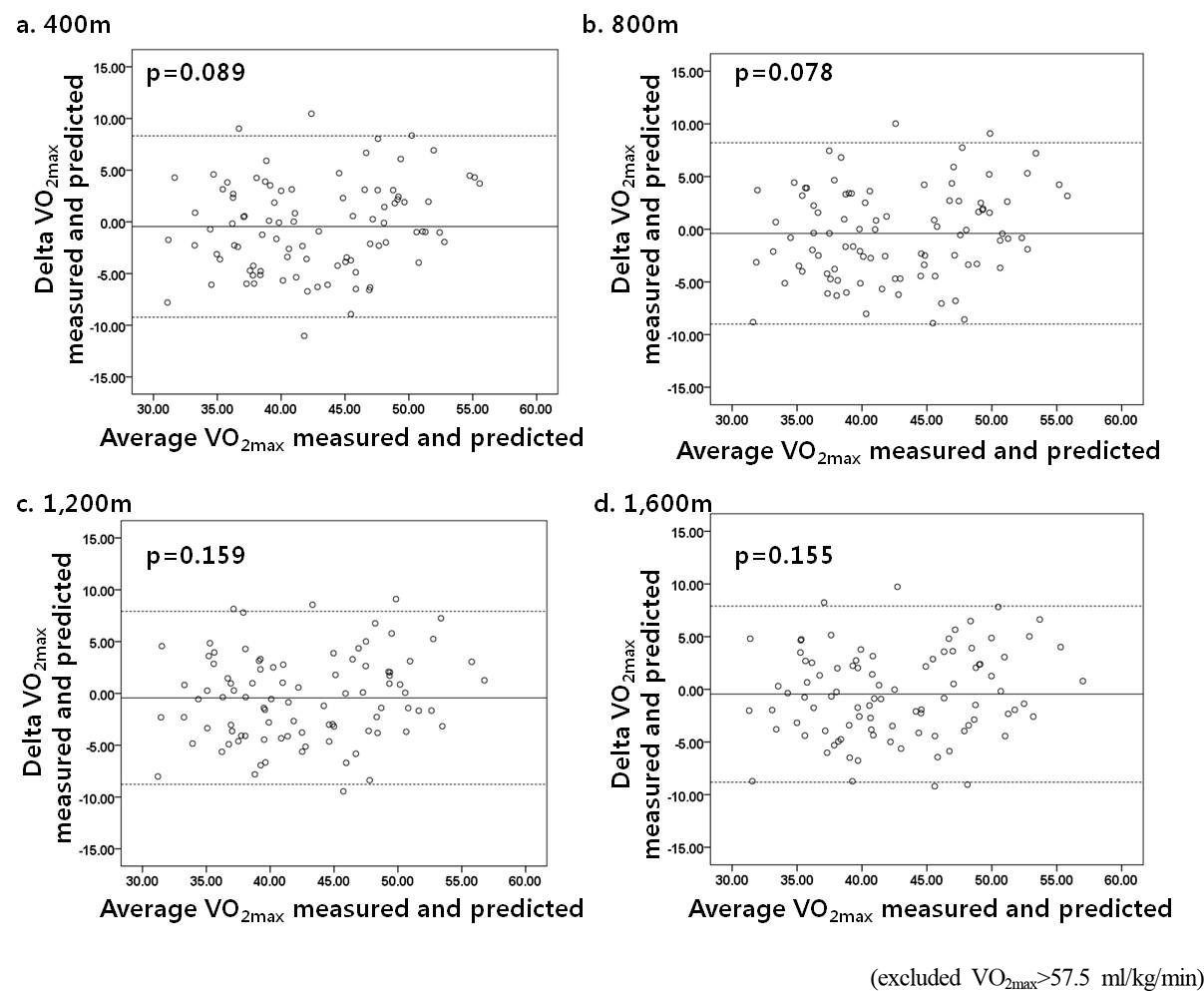
Bland-Altman plot of the measured and predicted VO2max with HR/ACM from pace controlled walk.

논의
스포츠의학 분야에서 체력요소 중 심폐지구력은 엘리트 선수의 호흡순환기능을 평가해 줄 수 있고, 질환자에게 임상적 의미를 전달해줄 수 있어 중요한 의미를 가진다. 또한 건강인의 유산소성능력을 평가해 줄 수 있다(Sartor et al., 2013). 본 연구는 필드테스트 시 운동강도에 대한 HR를 측정하고, 참여자의 측정 동기 및 운동능력에 상관없이 시행을 할 수 있는 객관적인 운동수행 기준을 도입하여 일반인이 일상생활에 쉽게 적용시킬 수 있으면서 타당도 높은 필드테스트를 개발하였다.
본 연구는 107명의 20대 남녀를 대상으로 시행하였다. 일반적으로 추정식 개발에 필요한 연구대상자 수는 변인 당 15~30명 또는 통계적 분석을 통해 결정하여야 한다(Palmer & OʼConnell, 2009). 타당한 대상자수를 산출하기 위해 G power 프로그램을 이용한 결과, 4개의 추정 변인 사용 시 총 85 명으로 필요한 대상자 수가 산출되어 본 연구의 대상자 수는 필드테스트 개발에 타당하다고 사료된다.
VO2max추정식 개발을 위한 추정변인
VO2max추정식 개발을 위한 추정변인을 채택하기 위하여 회귀분석 시 종속변수와 가장 높은 편상관관계를 갖는 변수를 선택하고 비유의적인 변수는 제거하기 위하여 단계선택(stepwise)방법으로 시행하였다. 신체적 특성 중 신장의 경우, VO2max와 상관관계 분석에서 유의하여 회귀분석의 변인으로 사용하였으나 성별이 회귀분석에 변인으로 들어감에 따라 유의도가 낮아져 변인으로는 채택되지 않았다. 체중도 시간이나 HR에 비해 유의도가 낮아 채택되지 않았다.
시간이나 거리, 속도, HR과 같은 운동 시 물리적 또는 생리적인 반응을 변인으로 사용하여 추정하는 경우 유전이나 환경요인이 더욱 고려될 수 있기 때문에 신체활동량에 대한 설문지나 신체구성을 이용하여 VO2max를 추정하는 간접법(George et al., 1997; Wier et al., 2006; Nes et al., 2011)보다 측정법의 타당성이 높아진다(George et al., 1997). 따라서 필드 테스트는 주로 일정거리나 일정시간 동안 운동 시행 후 시간, 거리, HR 등을 측정한다. 예를 들어, Rockport 1마일 걷기테스트는 1마일 걷기 시행 직후 측정된 시간과 HR로 VO2max를 추정한다(Kline et al., 1987). 본 연구는 운동능력에 상관없이 시행이 용이한 걷기 테스트(Rockport 1마일 걷기테스트)를 변형하여 메트로놈(bpm)을 이용한 일정 속도 걷기를 시행하였다. 일정속도 걷기에서 측정된 HR이 모든 구간(400 m, 800 m, 1,200 m, 1,600 m)에서 직접법에 의한 VO2max와 높은 상관이 나타났다. 하지만, HR은 신체활동 이외의 인자(유전, 연령, 운동습관, 복용 약물, 질환)의 영향을 받을 뿐만 아니라 운동부하가 불규칙하거나 HR이 항정 상태가 되지 않은 경우에 오차가 발생할 수 있다(Luke et al., 1997; Achten & Jeukendrup, 2003; Plasqui & Westerterp, 2005). 이에 운동강도에 대한 HR을 추정변인으로 사용하는 것이 제언되었다. Ambulatory foot-ground contact monitor를 이용하여 측정된 지면반력시간의 역수(1/tc)와 HR의 비(1/tcㆍHR)를 의미하는 aerobic fitness index (AFI)를 추정변인으로 사용한 경우 treadmill에서 자유롭게 선택한 속도(2~5 m/s)로 5분간의 달리기를 통해 측정되었다. AFI로 추정된 VO2max가 직접법의 VO2max와 상관이 나타나(r=0.84) 본 연구의 결과도 선행연구(Plasqui & Westerterp, 2006)와 비슷한 다중상관계수를 나타냈고, SEE는 4.7±0.8ml/kg/min로 신뢰도도 높았다(Weyand et al., 2001). 또한, 7일간의 일상생활 동안 측정한 HR과 ACM의 조합(HR/ACM)으로 산출한 지수를 사용한 VO2max추정식은 71% (R2)의 설명력을 가지며 %SEE는 13.7%로 나타났다(Plasqui & Westerterp, 2005). 따라서 운동능력이 높을수록 일정강도에 대한 HR은 낮게 나타나므로 이 지수만으로 운동능력을 평가할 수 있다(Oliver & Stembridge, 2011). 본 연구에서도 일정속도로 걷기 시 측정된 HR/ACM이 모든 구간(400 m, 800 m, 1,200 m, 1,600 m)에서 VO2max와 상관이 높게 나타났다.
HR을 이용하는 VO2max추정식은 시간을 추정변인으로 함께 사용되어야 한다. 걷기 시 HR과 시간이 역상관으로 나타나기 때문에 운동강도를 낮게 실시하여 HR이 낮아지더라도 시간이 증가하여 두 변인이 상호 보완된다(Kline et al., 1987). 본 연구의 일정속도로 걷기 시 측정된 시간이 모든 구간(400 m, 800 m, 1,200 m, 1,600 m)에서 VO2max와 유의한 상관이 나타났으며 단계적 회귀분석에서도 시간이 추정변인으로 채택되었다. 따라서 일정속도로 걷기 시 측정된 HR, HR/ACM, 그리고 시간이 VO2max추정식 개발을 위한 회귀분석의 독립변인으로 사용하는 것이 타당하다고 사료된다.
일정속도 걷기 시 VO2max추정식 및 타당도 분석
Plasqui 등(2005)은 일상생활 동안 측정한 활동강도에 대한 HR(HR/ACM)을 이용하여 VO2max를 추정하였다(Plasqui & Westerterp, 2005; Plasqui & Westerterp, 2006). 하지만 가속도계가 정적 활동을 측정할 수 없으며 HR이 감정이나 온도와 같은 외적 요인에 의해 영향을 받을 수 있기 때문에 HR과 ACM 측정에 있어서 제한점이 있다. 또한, 정확도를 위해 장기간(일주일) 측정을 하여야 한다. 따라서 본 연구에서는 짧은 시간 동안의 일정 속도 걷기테스트에 HR/ACM을 적용시켰다. 모든 구간에서 유의한 회귀식이 도출되었다. 또한, 타당도 분석 결과, 직접법에 의한 VO2max와 추정식에 의한 VO2max의 상관관계분석, PRESS 분석에서 유의한 상관관계가 나타났다. 또한, Bland-Altman plotting 분석 결과에서도 차이가 없는 것으로 나타났다. 즉, 140 bpm에 맞춰서 400 m를 걷는 것만으로도 VO2max를 추정할 수 있었다. 본 연구 결과 중 가장 짧은 거리의 방법은 400 m 일정속도로 걷기(HR/ACM 400 m)이며, 가장 높은 다중상관계수(R)를 나타냈던 것은 1,200 m 일정속도로 걷기였다(HR/ACM 1,200 m). 두 가지 회귀식은 Åstrand-Rhyming 자전거에르고미터 테스트, Rockport 1마일 걷기테스트와 비슷한 R, SEE, 그리고 %SEE가 나타났다..
걷기 시 구간별 HR, ACM, 시간 비교 분석
빠르게 걷기와 일정속도로 걷기 시 측정된 HR과 ACM, 그리고 시간을 비교한 결과, 빠르게 걷기보다 일정속도 걷기가 HR과 ACM이 낮게 나타났다. 따라서 일반인들이 일정속도로 걷기를 시행할 경우 빠르게 걷기에 비해 보다 수월하게 VO2max를 측정할 수 있을 것으로 판단된다. 실제로 %HRmax도 일정속도로 걷기에서 유의하게 낮게 나타나 일정속도로 걷기가 빠르게 걷기보다 저강도임을 확인할 수 있었다. 또한, 빠르게 걷기보다 일정속도로 걷기 시 더 많은 시간이 소요되었으나, 일정속도로 걷기(400 m)의 평균 시간은 3분 7초로 일반인들이 시행하기에 적당한 시간으로 사료된다. 따라서 일정속도로 걷기에서 나타난 저강도와 짧은 소요시간은 측정 시간이나 대상자의 동기 또는 운동능력과 같은 필드 테스트의 제한점을 해결해 줄 수 있을 것으로 판단된다(Lambrick et al., 2009).
가속도계에 따라서 activity count를 위한 센서 threshold에 차이가 있기 때문에 본 연구를 통해 개발된 VO2max추정식을 다른 가속도계에 직접 적용 시킬 수는 없지만, 현재 가속도계의 개발 방향은 모든 장비가 데이터를 공유할 수 있도록 표준화 작업이 진행되고 있다. 따라서 추후 표준화 threshold에 따라 기존에 개발된 추정식을 보정하는 연구가 필요할 것이다. 또한, 본 연구에 참여한 대상자의 직접법에 의한 VO2max의 범위는 27.2~63.5 ml/kg/min(여성은 27.2~52.4 ml/kg/min, 남성은 36~63.5 ml/kg/min)으로 체력수준이 다양하여 다양한 체력수준과 활동수준을 가진 20대 성인에게 적용시킬 수 있을 것으로 사료되며 추후 어린이 또는 30세 이상의 성인 또는 노인을 위한 측정법 개발이 요구된다.
측정목적에 따라 측정법 선택 시 고려사항이 달라진다. 전문 스포츠 영역에서는 트레이닝에 의한 변화를 측정할 수 있는 점이 중요하며, 임상의학 영역에서는 측정 시 HR, 혈압, 운동량 등 여러 생리적인 변인을 측정할 수 있어야 한다(ACSM, 2010; Sartor et al., 2013). 그러나 일반인의 건강체력 평가를 위해서는 측정방법이 특별한 지도 없이 시행할 수 있어야 하며 소요시간도 적당해야 한다(Sartor et al., 2013; Sartor et al., 2013; Evans et al., 2014). 따라서 본 연구를 통해 개발된 4개의 추정식은 측정환경에 따라서 적절하게 측정방법을 선택할 수 있을 것으로 사료된다. 그 중 400 m 일정속도 걷기(HR/ACM400 m)는 단시간(평균 4 분)에 최대 하 운동강도(평균 69%HRmax)의 걷기를 통해 VO2max를 평가할 수 있으므로 일반인들이 쉽게 VO2max를 측정할 수 있을 것이다.
결론 및 제언
본 연구는 신뢰도와 타당도, 경제성이 높은 심폐지구력 측정방법을 개발하기 위해 일정속도로 걷기(pace controlled walk)시의 HR/ACM을 이용한 VO2max추정식을 산출하고 그 타당도를 비교 검토하였다. 그 결과, 직접법에 의한 VO2max는 일정속도로 걷기 시 HR/ACM 또는 걷기시간과 유의한 상관관계가 나타났다. 또한 HR/ACM을 추정변인으로 하여 일정속도로 걷기 시 400 m 걷기만으로 VO2max추정이 가능하였다. 추정식은 다음과 같으며 이때 R2은 0.675, %SEE는 10.7로 나타났다. VO2max=121.659 +6.656×Gender-0.865×Age-9.540×Time–2460.952×HR/ACM (Gender, 0=female, 1= male: Time, hundredth of a minute: HR, heart rate: ACM, activity count per minute)
이상의 결과로부터 심박수와 가속도계를 함께 사용할 경우 400 m 일정속도 걷기(HR/ACM400 m)를 통해 VO2max를 추정할 수 있었다. 따라서 bpm에 맞춰 쉽게 그리고 보다 짧은 거리의 걷기를 통해 일반인의 체력측정이 가능할 것으로 사료된다. 본 연구에서는 20대 성인에 대해서만 시행하였으나, 추후에는 다양한 bpm을 설정하여 보다 수행하기 용이하며 타당도를 높일 수 있는 추정식 개발이 요구된다.
Acknowledgements
본 논문은 2015년도 ㈜LG전자의 지원을 받아 연구되었음.
References
Achten, J. & Jeukendrup, A. E. (2003). Heart rate monitoring: applications and limitations. Sports Medicine, 33(7), 517-538.
Achten J., et al, Jeukendrup A. E.. 2003;Heart rate monitoring: applications and limitations. Sports Medicine 33(7):517–538.American College of Sports Medicine. (2010). ACSMʼs Guidelines for Exercise Testing and Prescription: Lippincott Williams and Wilkins: Philadelphia, PA.
American College of Sports Medicine. 2010. ACSMʼs Guidelines for Exercise Testing and Prescription Lippincott Williams and Wilkins. Philadelphia, PA:Åstrand, P. O. & Ryhming, I. (1954). A nomogram for calculation of aerobic capacity(physical fitness) from pulse rate during sub-maximal work.Journal of Applied Physiology, 7(2), 218-221.
Åstrand P. O., et al, Ryhming I.. 1954;A nomogram for calculation of aerobic capacity(physical fitness) from pulse rate during sub-maximal work. Journal of Applied Physiology 7(2):218–221. 10.1152/jappl.1954.7.2.218.Bland, J. M. & Altman, D. G. (1986). Statistical methods for assessing agreement between two methods of clinical measurement. The Lancet, 327(8476), 307-310.
Bland J. M., et al, Altman D. G.. 1986;Statistical methods for assessing agreement between two methods of clinical measurement. The Lancet 327(8476):307–310.Borg, G. A. (1973). Perceived exertion: a note on "history" and methods. Medicine and Science in Sports, 5(2), 90-93.
Borg G. A.. 1973;Perceived exertion: a note on "history" and methods. Medicine and Science in Sports 5(2):90–93.Bruce, R. A. & McDonough, J. R. (1969). Stress testing in screening for cardiovascular disease. Bulletin of the New York Academy of Medicine, 45(12), 1288-1305.
Bruce R. A., et al, McDonough J. R.. 1969;Stress testing in screening for cardiovascular disease. Bulletin of the New York Academy of Medicine 45(12):1288–1305.Butte, N. F., Ekelund, U., & Westerterp, K. R. (2012). Assessing physical activity using wearable monitors: measures of physical activity. Medicine and Science in Sports and Exercise, 44(1 Suppl 1), S5-12.
Butte N. F., Ekelund U., et al, Westerterp K. R.. 2012;Assessing physical activity using wearable monitors: measures of physical activity. Medicine and Science in Sports and Exercise 44(1 Suppl 1):S5–12.Cao, Z. B., Miyatake, N., Higuchi, M., Miyachi, M., Ishikawa-Takata, K., & Tabata, I. (2010). Predicting VO2max with an objectively measured physical activity in Japanese women. Medicine and Science in Sports and Exercise, 42(1), 179-186.
Cao Z. B., Miyatake N., Higuchi M., Miyachi M., Ishikawa-Takata K., et al, Tabata I.. 2010;Predicting VO2max with an objectively measured physical activity in Japanese women. Medicine and Science in Sports and Exercise 42(1):179–186. 10.1249/mss.0b013e3181af238d.Choi, H. M., Kim, J. K., Chun, J. M., Yang, S. W., & Nho, H. S. (2011). Validation of a Activity Tracker for Assessing Energy Expenditure. The Korea Journal of Sports Science, 20(6), 1251-1260.
Choi H. M., Kim J. K., Chun J. M., Yang S. W., et al, Nho H. S.. 2011;Validation of a Activity Tracker for Assessing Energy Expenditure. The Korea Journal of Sports Science 20(6):1251–1260.Evans, H. J., Ferrar, K. E., Smith, A. E., Parfitt, G., & Eston, R. G. (2014). A systematic review of methods to predict maximal oxygen uptake from submaximal, open circuit spirometry in healthy adults. Journal of Science and Medicine in Sport. 18(3), 183-188.
Evans H. J., Ferrar K. E., Smith A. E., Parfitt G., et al, Eston R. G.. 2014;A systematic review of methods to predict maximal oxygen uptake from submaximal, open circuit spirometry in healthy adults. Journal of Science and Medicine in Sport 18(3):183–188.Evans, H. J., Parfitt, G., & Eston, R. G. (2013). The perceptually regulated exercise test is sensitive to increases in maximal oxygen uptake. European Journal of Applied Physiology, 113(5), 1233-1239.
Evans H. J., Parfitt G., et al, Eston R. G.. 2013;The perceptually regulated exercise test is sensitive to increases in maximal oxygen uptake. European Journal of Applied Physiology 113(5):1233–1239. 10.1007/s00421-012-2541-3.Faul, F., Erdfelder, E., Lang, A. G., & Buchner, A. (2007). G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior research methods, 39(2), 175-191.
Faul F., Erdfelder E., Lang A. G., et al, Buchner A.. 2007;G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior research methods 39(2):175–191. 10.3758/bf03193146.Fudge, B. W., Wilson, J., Easton, C., Irwin, L., Clark, J., Haddow, O., Kayser, B., & Pitsiladis, Y. P. (2007). Estimation of oxygen uptake during fast running using accelerometry and heart rate. Medicine and Science in Sports and Exercise, 39(1), 192-198.
Fudge B. W., Wilson J., Easton C., Irwin L., Clark J., Haddow O., Kayser B., et al, Pitsiladis Y. P.. 2007;Estimation of oxygen uptake during fast running using accelerometry and heart rate. Medicine and Science in Sports and Exercise 39(1):192–198. 10.1249/01.mss.0000235884.71487.21.George, J. D., Stone, W. J., & Burkett, L. N. (1997). Non-exercise VO2max estimation for physically active college students. Medicine and Science in Sports and Exercise, 29(3), 415-423.
George J. D., Stone W. J., et al, Burkett L. N.. 1997;Non-exercise VO2max estimation for physically active college students. Medicine and Science in Sports and Exercise 29(3):415–423. 10.1097/00005768-199703000-00019.Grossman, R. F., Frost, A., Zamel, N., Patterson, G. A., Cooper, J. D., Myron, P. R., Dear, C. L., & Maurer, J. (1990). Results of single-lung transplantation for bilateral pulmonary fibrosis. New England Journal of Medicine, 322(11), 727-733.
Grossman R. F., Frost A., Zamel N., Patterson G. A., Cooper J. D., Myron P. R., Dear C. L., et al, Maurer J.. 1990;Results of single-lung transplantation for bilateral pulmonary fibrosis. New England Journal of Medicine 322(11):727–733. 10.1056/nejm199003153221104.Holiday, D. B., Ballard, J. E., & McKeown, B. C. (1995). PRESS-related statistics: regression tools for cross-validation and case diagnostics. Medicine and Science in Sports and Exercise, 27(4), 612-620.
Holiday D. B., Ballard J. E., et al, McKeown B. C.. 1995;PRESS-related statistics: regression tools for cross-validation and case diagnostics. Medicine and Science in Sports and Exercise 27(4):612–620.Howley, E. T., Bassett, D. R., Jr., & Welch, H. G. (1995). Criteria for maximal oxygen uptake: review and commentary. Medicine and Science in Sports and Exercise, 27(9), 1292-1301.
Howley E. T., Bassett D. R. Jr., et al, Welch H. G.. 1995;Criteria for maximal oxygen uptake: review and commentary. Medicine and Science in Sports and Exercise 27(9):1292–1301.Katzmarzyk, P. T., Church, T. S., & Blair, S. N. (2004). Cardiorespiratory fitness attenuates the effects of the metabolic syndrome on all-cause and cardiovascular disease mortality in men. Archives of Internal Medicine, 164(10), 1092-1097.
Katzmarzyk P. T., Church T. S., et al, Blair S. N.. 2004;Cardiorespiratory fitness attenuates the effects of the metabolic syndrome on all-cause and cardiovascular disease mortality in men. Archives of Internal Medicine 164(10):1092–1097. 10.1001/archinte.164.10.1092.Kavanagh, J. J. & Menz, H. B. (2008). Accelerometry: a technique for quantifying movement patterns during walking. Gait Posture, 28(1), 1-15.
Kavanagh J. J., et al, Menz H. B.. 2008;Accelerometry: a technique for quantifying movement patterns during walking. Gait Posture 28(1):1–15. 10.1016/j.gaitpost.2007.10.010.Kline, G. M., Porcari, J. P., Hintermeister, R., Freedson, P. S., Ward, A., McCarron, R. F., Ross, J., & Rippe, J. M. (1987). Estimation of VO2max from a one-mile track walk, gender, age, and body weight. Medicine and Science in Sports and Exercise, 19(3), 253-259.
Kline G. M., Porcari J. P., Hintermeister R., Freedson P. S., Ward A., McCarron R. F., Ross J., et al, Rippe J. M.. 1987;Estimation of VO2max from a one-mile track walk, gender, age, and body weight. Medicine and Science in Sports and Exercise 19(3):253–259.Kodama, S., Saito, K., Tanaka, S., Maki, M., Yachi, Y., Asumi, M., Sugawara, A., Totsuka, K., Shimano, H., Ohashi, Y., Yamada, N., & Sone, H. (2009). Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. The Journal of the American Medical Association, 301(19), 2024-2035.
Kodama S., Saito K., Tanaka S., Maki M., Yachi Y., Asumi M., Sugawara A., Totsuka K., Shimano H., Ohashi Y., Yamada N., et al, Sone H.. 2009;Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. The Journal of the American Medical Association 301(19):2024–2035.Kumahara, H., Schutz, Y., Ayabe, M., Yoshioka, M., Yoshitake, Y., Shindo, M., Ishii, K., & Tanaka, H. (2004). The use of uniaxial accelerometry for the assessment of physical-activity-related energy expenditure: a validation study against whole-body indirect calorimetry. The British Journal of Nutrition, 91(2), 235-243.
Kumahara H., Schutz Y., Ayabe M., Yoshioka M., Yoshitake Y., Shindo M., Ishii K., et al, Tanaka H.. 2004;The use of uniaxial accelerometry for the assessment of physical-activity-related energy expenditure: a validation study against whole-body indirect calorimetry. The British Journal of Nutrition 91(2):235–243. 10.1079/bjn20031033.Lambrick, D. M., Faulkner, J. A., Rowlands, A. V., & Eston, R. G. (2009). Prediction of maximal oxygen uptake from submaximal ratings of perceived exertion and heart rate during a continuous exercise test: the efficacy of RPE 13. European Journal of Applied Physiology, 107(1), 1-9.
Lambrick D. M., Faulkner J. A., et al, Rowlands A. V., et al, Eston R. G.. 2009;Prediction of maximal oxygen uptake from submaximal ratings of perceived exertion and heart rate during a continuous exercise test: the efficacy of RPE 13. European Journal of Applied Physiology 107(1):1–9. 10.1007/s00421-009-1093-7.Luke, A., Maki, K. C., Barkey, N., Cooper, R., & McGee, D. (1997). Simultaneous monitoring of heart rate and motion to assess energy expenditure. Medicine and Science in Sports and Exercise, 29(1), 144-148.
Luke A., Maki K. C., Barkey N., Cooper R., et al, McGee D.. 1997;Simultaneous monitoring of heart rate and motion to assess energy expenditure. Medicine and Science in Sports and Exercise 29(1):144–148. 10.1097/00005768-199701000-00021.Nes, B. M., Janszky, I., Vatten, L. J., Nilsen, T. I., Aspenes, S. T., & Wisloff, U. (2011). Estimating VO2peak from a nonexercise prediction model: the HUNT Study, Norway. Medicine and Science in Sports and Exercise, 43(11), 2024-2030.
Nes B. M., Janszky I., Vatten L. J., Nilsen T. I., Aspenes S. T., et al, Wisloff U.. 2011;Estimating VO2peak from a nonexercise prediction model: the HUNT Study, Norway. Medicine and Science in Sports and Exercise 43(11):2024–2030.Oliver, J. L. & Stembridge, M. (2011). Use of a heart rate-to-ground contact time index to monitor and predict middle-distance running. European Journal of Sport Science, 11(6), 431-436.
Oliver J. L., et al, Stembridge M.. 2011;Use of a heart rate-to-ground contact time index to monitor and predict middle-distance running. European Journal of Sport Science 11(6):431–436. 10.1080/17461391.2010.536582.Palmer, P. B. & OʼConnell, D. G. (2009). Regression analysis for prediction: understanding the process. Cardiopulmonary Physical Therapy Journal, 20(3), 23-26.
Palmer P. B., et al, OʼConnell D. G.. 2009;Regression analysis for prediction: understanding the process. Cardiopulmonary Physical Therapy Journal 20(3):23–26.Plasqui, G. & Westerterp, K. R. (2005). Accelerometry and heart rate as a measure of physical fitness: proof of concept. Medicine and Science in Sports and Exercise, 37(5), 872-876.
Plasqui G., et al, Westerterp K. R.. 2005;Accelerometry and heart rate as a measure of physical fitness: proof of concept. Medicine and Science in Sports and Exercise 37(5):872–876. 10.1249/01.mss.0000161805.61893.c0.Plasqui, G. & Westerterp, K. R. (2006). Accelerometry and heart rate as a measure of physical fitness: cross-validation. Medicine and Science in Sports and Exercise, 38(8), 1510-1514.
Plasqui G., et al, Westerterp K. R.. 2006;Accelerometry and heart rate as a measure of physical fitness: cross-validation. Medicine and Science in Sports and Exercise 38(8):1510–1514.Powers, S. K. & Howley, E. T. (2008). Exercise Physiology: Theory and Application to Fitness and Performance (Sixth ed.): McGraw-Hill.
Powers S. K., et al, Howley E. T.. 2008. Exercise Physiology: Theory and Application to Fitness and Performance Sixth edth ed. McGraw-Hill.Rowlands, A. V., Stone, M. R., & Eston, R. G. (2007). Influence of speed and step frequency during walking and running on motion sensor output. Medicine and Science in Sports and Exercise, 39(4), 716-727.
Rowlands A. V., Stone M. R., et al, Eston R. G.. 2007;Influence of speed and step frequency during walking and running on motion sensor output. Medicine and Science in Sports and Exercise 39(4):716–727. 10.1249/mss.0b013e318031126c.Sartor, F., Vernillo, G., de Morree, H. M., Bonomi, A. G., La Torre, A., Kubis, H. P., & Veicsteinas, A. (2013). Estimation of maximal oxygen uptake via submaximal exercise testing in sports, clinical, and home settings. Sports Medicine, 43(9), 865-873.
Sartor F., Vernillo G., de Morree H. M., Bonomi A. G., La Torre A., Kubis H. P., et al, Veicsteinas A.. 2013;Estimation of maximal oxygen uptake via submaximal exercise testing in sports, clinical, and home settings. Sports Medicine 43(9):865–873. 10.1007/s40279-013-0068-3.Treuth, M. S., Schmitz, K., Catellier, D. J., McMurray, R. G., Murray, D. M., Almeida, M. J., Going, S., Norman, J. E., & Pate, R. (2004). Defining accelerometer thresholds for activity intensities in adolescent girls. Medicine and Science in Sports and Exercise, 36(7), 1259-1266.
Treuth M. S., Schmitz K., Catellier D. J., McMurray R. G., Murray D. M., Almeida M. J., Going S., Norman J. E., et al, Pate R.. 2004;Defining accelerometer thresholds for activity intensities in adolescent girls. Medicine and Science in Sports and Exercise 36(7):1259–1266.Wei, M., Kampert, J. B., Barlow, C. E., Nichaman, M. Z., Gibbons, L. W., Paffenbarger, R. S., Jr., & Blair, S. N. (1999). Relationship between low cardiorespiratory fitness and mortality in normal-weight, overweight, and obese men. The Journal of the American Medical Association, 282(16), 1547-1553.
Wei M., Kampert J. B., Barlow C. E., Nichaman M. Z., Gibbons L. W., Paffenbarger R. S. Jr, et al, Blair S. N.. 1999;Relationship between low cardiorespiratory fitness and mortality in normal-weight, overweight, and obese men. The Journal of the American Medical Association 282(16):1547–1553. 10.1001/jama.282.16.1547.Westerterp, K. R. & Bouten, C. V. (1997). Physical activity assessment: comparison between movement registration and doubly labeled water method. Zeitschrift fur Ernahrungswissenschaft, 36(4), 263-267.
Westerterp K. R., et al, Bouten C. V.. 1997;Physical activity assessment: comparison between movement registration and doubly labeled water method. Zeitschrift fur Ernahrungswissenschaft 36(4):263–267. 10.1007/bf01617795.Weyand, P. G., Kelly, M., Blackadar, T., Darley, J. C., Oliver, S. R., Ohlenbusch, N. E., Joffe, S. W., & Hoyt, R. W. (2001). Ambulatory estimates of maximal aerobic power from foot-ground contact times and heart rates in running humans. Journal of Applied Physiology, 91(1), 451-458.
Weyand P. G., Kelly M., Blackadar T., Darley J. C., Oliver S. R., Ohlenbusch N. E., Joffe S. W., et al, Hoyt R. W.. 2001;Ambulatory estimates of maximal aerobic power from foot-ground contact times and heart rates in running humans. Journal of Applied Physiology 91(1):451–458. 10.1152/jappl.2001.91.1.451.Wier, L. T., Jackson, A. S., Ayers, G. W., & Arenare, B. (2006). Non exercise models for estimating VO2max with waist girth, percent fat, or BMI. Medicine and Science in Sports and Exercise, 38(3), 555-561.
Wier L. T., Jackson A. S., Ayers G. W., et al, Arenare B.. 2006;Non exercise models for estimating VO2max with waist girth, percent fat, or BMI. Medicine and Science in Sports and Exercise 38(3):555–561.