여성 선수의 상대적 에너지 결핍에 대한 최신 지견
Recent Advance on Relative Energy Deficiency in Female Athlete
Article information
Abstract
[목적]
본 종설의 목적은 상대적에너지결핍(relative energy deficiency in sports; RED-S)와 낮은 에너지가용성(low energy availability; LEA)로 인해 운동선수에서 나타날 수 있는 건강학적 문제와 예방에 대한 최근 연구 동향을 정리하였다.
[방법]
본 종설을 위해 ‘PubMed’, ‘Google Scholar’, ‘Science Direct databases’와 같은 학술 검색 시스템을 활용하여 연구 논문을 자료로 수집하였다.
[결과]
에너지 가용성(energy availability; EA)는 섭취열량에서 운동으로 사용한 에너지를 제외한 양을 의미하며, 낮은 에너지 가용성(low energy availability; LEA)은 RED-S의 surrogate marker로 여겨지고 있다. 여러 선행연구에서, 여성 선수들에서 만성적인 가용에너지의 부족은 시상하부-뇌하수체-성선(HPC) 축과 뼈 건강을 넘어 내분비 기능장애, 면역기능저하, 심리학적 장애와 같은 건강학적 문제를 초래할 뿐만 아니라 부상위험의 증가, 운동수행력 감소가 나타날 수 있다고 제시하고 있다.
[결론]
RED-S로 초래된 건강악화는 회복이 어려울 수 있기때문에 관련 징후의 조기발견 및 예방이 매우 중요하다. 따라서 선수, 지도자 및 부모에게 RED-S와 관련된 다양한 증상으로 인한 문제점을 인지할 수 있는 교육 프로그램 개발 및 교육 중재가 중요하다.
Trans Abstract
PURPOSE
The purpose of this review was to summarize the current knowledge on the trends in athletes’ health problems (and their preventive strategies) caused by low energy availability (LEA) and relative energy deficiency in sports (RED-S).
METHODS
In this narrative review, we summarized previous studies by searching the literature in the PubMed, Google Scholar, and Science Direct databases.
RESULTS
Energy availability (EA) refers to the amount of energy from caloric intake used for exercise, and a LEA is considered as a surrogate marker of RED-S. In several previous studies, chronic low energy availability in female athletes has been reported to cause health problems such as endocrine dysfunctions, immunosuppression, and psychological disorders, and to also affect the hypothalamic-pituitary-gonadal (HPC) axis and bone health. Moreover, it has been suggested that an increase in injury risk and a decrease in exercise performance may occur.
CONCLUSIONS
Since it can be difficult to recover from the health deteriorations caused by RED-S, early detection (of related signs and symptoms) and prevention are very important. Therefore, athletes, coaches, and parents need to develop educational programs that ease the recognition of the problems caused by various symptoms related to RED-S and promote educational interventions.
서론
많은 선수들에게 상대적 에너지 결핍(Relative Energy Deficiency in Sport; RED-S)은 아직 생소한 용어일 수 있다. 그렇기 때문에 다수의 선수들이 RED-S 관련 증상을 경험하고도 그 심각성을 알지 못해 그냥 방치하는 경우가 대부분일 것이다.
RED-S는 2014년 국제 올림픽 위원회(IOC)에 의해 처음 도입된 이래(Mountjoy et al., 2014), 2018년에 또 다른 IOC 합의에 의해 업데이트되었다(Mountjoy et al., 2018). RED-S는 낮은 에너지 가용성(low energy availability; LEA)으로 인해 발생하며(Mountjoy et al., 2014; Slater et al., 2017) 주요 증상으로 여성 선수에 월경 장애와 뼈의 건강 악화를 들 수 있으며, 이는 삼징후(traid)로 알려져 있다. RED-S는 LEA로 인한 복합 증후군으로 정의되어 생리 기능 장애를 초래하여 건강 및 수행 측면에 부정적인 영향을 미친다. RED-S의 개념은 선수들에게서의 만성적인 가용에너지 부족이 시상하부-뇌하수체-성선(HPG) 축과 뼈 건강을 넘어 건강에 부정적인 결과를 초래할 수 있다는 전제를 뒷받침하는 새로운 과학적 근거들의 축적으로 이루어졌다. IOC의 RED-S 합의문에서는 만성적인 LEA가 잠재적으로 다양한 신체 시스템에 영향을 미쳐 부정적인 건강 및 수행 결과를 초래하는 방법을 보여주고 기존의 삼징후와의 관계를 나타내기 위한 도식을 개발하였다(Mountjoy et al., 2014).
만성적인 가용에너지 부족으로 인해 내분비 기능장애, 면역기능저하, 체지방 증가 및 근육량 감소뿐만 아니라 부상위험증가, 운동수행력 및 트레이닝 효과 감소가 나타날 수 있다(Ackerman et al., 2019). 선수들에서 나타나는 일반적인 가용에너지 부족은 운동으로 소모되는 열량보다 음식섭취 열량이 상대적으로 작을 때 나타나게 되는 데 그렇기 때문에 체중관리를 해야 하는 무용수나 심미적 스포츠, 체급 및 장거리 육상과 같은 기록경기 선수들에게서 더 나타날 가능성이 높다(Nattiv et al., 2007). RED-S로 초래된 건강악화는 회복이 어려울 수 있기 때문에 관련 징후의 조기발견 및 예방이 매우 중요하다. 이에 IOC와 ACSM에서는 진단도구를 개발하여 여성선수들의 RED-S 예방을 위해 만 18세 이전부터 년 1~2회 자가진단을 권고하고 있으며, 선수들의 스포츠 참가 허용 밑 부상 후 회복을 결정하는 데 사용하도록 권고하고 있다(De Souza et al., 2014; Mountjoy et al., 2014).
본 종설에서는 RED-S/LEA로 인해 여성운동선수에서 나타날 수 있는 건강학적 문제와 예방에 대한 최근 연구 동향을 정리해 보았다.
연구방법
자료 수집
본 종설의 작성을 위해 ‘PubMed’, ‘Google Scholar’, ‘Science Direct databases’와 같은 학술 검색 시스템을 활용하여 연구 논문을 자료로 수집하였다. 검색 키워드는 ‘relative energy deficiency in sport’, ‘low energy availability’, ‘female athlete triad-relative energy deficiency in sport’, ‘female athlete triad’ 등으로 문헌을 검색하였다.
연구결과
여자선수 3징후 vs. 상대적 에너지 결핍
트레이닝을 통해 소모되는 열량보다 섭취하는 열량이 적을 경우 체내 가용에너지는 부족해진다. 체내 가용에너지 부족현상은 체중감량을 목적으로 의도적으로 식이 섭취량을 제한할 경우 또는 식이장애가 있을 경우 더욱 심해질 수 있으며, 의도적인 식이섭취량 제한 없이 트레이닝량 만큼 식이를 충분히 섭취하지 않을 경우 비의도적으로 발생할 수 있다. 이러한 체내 에너지 부족 현상이 지속될 경우 여자선수에서 월경장애, 골밀도 저하가 서로 관련지어 나타나는데, 1992년 미 스포츠 의학회(ACSM)는 식이장애 유무에 상관없이 나타나는 가용에너지 부족, 월경장애, 낮은 골밀도 3가지 현상을 일으켜 ‘여자선수 3징후(Female Athlete Triad; FAT)’으로 정의하였다(Otis et al., 1997). 앞에서 언급한 바와 같이 3가지 요인은 서로 밀접하게 관련되어 있기 때문에 하나라도 증상이 있다면 FAT으로 진단된다. 여자 운동선수들은 3가지 요인 중 하나 또는 하나 이상 증상을 갖고 있는 경우가 많으며, 주로 무용수나 심미적 스포츠 분야(체조, 다이빙, 피겨 스케이팅 등), 체급 스포츠 분야(레슬링, 복싱, 유도, 태권도 등) 그리고 장거리 육상선수들에서 자주 관찰된다. 이후 2007년 ACSM은 공식적인 입장을 수정하여 식이 장애 유무에 상관없이 나타나는 낮은 가용에너지(low energy availability; LEA)를 FAT 유발 원인으로 지목하였고, FAT의 세 가지 요인을 LEA, 기능성 시상하부 무월경(functional hypothalamic amenorrhea; FHA), 골다공등으로 수정하였다(Nattiv et al., 2007)(Figure 1). 이러한 FAT의 요소들은 최적의 건강 상태에서 임상적 질병상태까지 연속적이고 입체적인 개념으로 여겨지고 있으며, 선수들이 심각한 임상 상태로 진행되지 전 예방 및 조기 치료의 중요성을 강조하였다.

Schematic of the components of the female athlete triad, a spectrum disorder, based on the updated 2007 guidelines. (Modified from source: Nattiv et al., MSSE 2007)
2014년 IOC에서는 FAT을 스포츠 상황에서의 상대적 에너지 부족(Relative Energy Deficienc in Sportl; RED-S)이라는 이름으로 새로 정의하였으며, RED-S 개념에서 상대적 에너지 부족은 여성 뿐만 아니라 남성에서도 나타날 수 있고, 월경기능, 뼈 건강 뿐만 아니라 더 다양한 체내 생리적 기능 및 경기력에도 영향을 미치고 있음을 제시하고 있다(Mountjoy et al., 2018)(Figure 2). RED-S와 FAT을 정의한 단체와 명칭은 다르지만 두 용어 모두 체내 에너지 결핍현상 즉 ‘낮은 가용에너지(low energy availability)가 선수들의 건강 악화 및 신체적 기능 저하의 주요 발생요인’이라는 점을 동일하게 제시하고 있으며, 선수들의 건강 및 경기력을 위해 가용에너지의 중요성에 대해 강조하고 있다.

Health and performance consequence of Relative Energy Deficiency in Sport (RED-S). (*Psychological consequences can either precede RED-S or be the results of RED-S). (Modified from source: Mountjoy et al., IJSNEM 2018)
낮은 에너지 가용성
지난 30여 년간, 여자 운동선수에서 빈번하게 관찰되는 생리기능장애, 낮은 골밀도에 대한 원인을 밝히고자 많은 연구가 이루어져 왔으며, 낮은 에너지 가용성(low energy availability; LEA)는 RED-S의 surrogate marker로 여겨지고 있다. 에너지 가용성(energy availability; EA)는 섭취열량에서 운동으로 사용한 에너지를 제외한 양을 의미하며(Nattiv et al., 2007), 이는 아래의 공식과 같이 신체 크기가 서로 다른 사람들의 가용 에너지 상태를 비교하기 위해 제지방량으로 나눈다(Manore et al., 2007).
가용에너지 = 식이섭취량 – 운동에너지 소비량/제지방량
모든 생리적 기능을 적절하게 유지하기 위해 가용에너지는 적어도 88KJ(45kcal/kg fat-free mass/day) 정도가 필요하다. 125-188KJ(30-45kcal)/kg/fat free mass/day는 가용에너지가 감소된 또는 준 임상적 상태이며, 이는 체중 감량을 목표로 하는 운동선수들에게 단기간 동안 허용 가능한 범위이다. 가용에너지 수준 125KJ(30kcal)/kg/fat free mass/day 이하는 호르몬 축 교란을 유발시키게 되는 가용에너지의 경계값으로써 이 에너지 수준은 최적의 신체 기능을 수행하기에 안전한 상태가 아니라고 판단할 수 있다. 가용에너지가 30kcal/kg/fat free mass/day 이하로 감소될 때 가장 많이 알려진 신체에 미치는 부적적인 영향은 생식기능 및 골대사 기능 저하이다(Loucks & Thuma, 2003; Ihle & Loucks, 2004). LEA는 고의적인 임상적 식이장애 또는 이상섭식행동으로 발생할 수도 있고, 적절한 식이 섭취에 대한 인식부족으로 의도치 않게 발생할 수도 있다(Nattiv et al., 2007; Mountjoy et al., 2014). 가용에너지의 병인론에 따르면, 낮은 가용에너지는 다량 그리고 미량 에너지 부족을 일으킬 수 있으며, 부정적인 생리적 변화를 가져와 잠재적으로 건강 및 스포츠 경기력에 악영향을 미칠 수 있다. 그러나 최근 연구에 따르면 이 임계치가 모든 여자들의 무월경을 예측하는 것은 아니라고 제시하고 있지만(Lieberman et al., 2018; Williams et al., 2015) 신체 크기와 사춘기 연령 차이를 따지지 않는다면 30 kcal/kg FFM/day는 대략 평균 안정시 대사율(RMR)과 유사한 수준이다(Loucks et al., 2011). LEA은 실험실 연구(Loucks & Heath, 1994; Loucks & Thuma, 2003) 및 현장연구(Melin et al., 2014; Vanheest et al., 2014)에서 모두 최적에 미달하는 건강상태과 기능에 대한 지표로서 입증되었기 때문에 에너지 가용성 평가는 RED-S 예방 및 관리에 대한 진단적 도구에서 의미가 있을 것으로 사료된다. LEA는 마름을 추구하는 특정 스포츠 뿐만 아니라 다양한 스포츠에서 나타나고 있고 있지만(Pollock et al., 2010; Schtscherbyna et al., 2009; Martinsen et al., 2010), 운동선수 그룹 특성에 따라 예를 들어 운동수행력이나 연령에 따라 매우 다르게 나타나며, 적은 샘플 사이즈도 정확도에 영향을 미친다. 따라서 낮은 가용에너지의 유병률을 더 잘 이해하기 위해 남녀 모두 그리고 모든 스포츠에 걸친 높은 증거수준을 제시할 만한 연구가 필요하다.
1. 에너지 가용성 평가방법
운동선수가 적절한 가용에너지를 보유하고 있는지를 평가하는 것이 가장 중요하지만, 현재까지 가용에너지를 평가하는 표준 지표는 없는 실정이다. 일반적으로 섭취에너지와 운동 중 에너지 소모량을 측정하고 있으나 이에 대한 표준화된 프로토콜도 없으며(예를 들어, 수집일수, 섭취 에너지 평가 방법, 운동 에너지 또는 제지방량 평가 방법), 각 측정항목의 신뢰성과 타당도가 부족하다. 에너지 가용성을 평가하는 가장 중요한 점은 자가 보고에서 섭취 에너지량을 정확하게 기록하는 것이며(Burke & Deakin, 2015; Burke et al., 2018), 운동선수가 수행하는 많은 훈련, 경기 활동 중 에너지 소모량을 측정하고, 추가적인 레크리에이션 및 생활 속 활동들도 포함해야 한다는 것이다(Burke & Deakin, 2015; Cialdella-Kam et al., 2014). 이러한 문제점들은 현장 연구에서 계산된 가용에너지와 관련 증상 사이에 상당한 불일치가 나타나는 것으로 설명될 수 있다. 그러나 자가보고 형식의 회상 식이 설문지는 4일 후부터 순응도가 감소되며(Magkos & Yannakoulia, 2003), 몇몇 연구자들이 정확한 식이 로그를 유지하기 위해 운동선수들을 교육하고, 규칙적으로 체크함으로써 이에 대한 문제점들을 극복하고자 노력해왔다(Reed et al., 2013; Reed et al., 2014). 또한 식이 섭취와 운동을 평가하는 기간의 불일치, 특정 식이 성분들(섬유질 과다섭취, 자극적인 인공감미료, 낮은 에너지 밀도, 과도한 식이 통제, 하루 중 불균형한 에너지 섭취)는 낮은 가용에너지의 영향을 가속화할 수 있다(Barron et al., 2015; Gaskins et al., 2009; Heikura et al., 2018; Melin et al., 2016; Reed et al., 2014). 이러한 문제가 해결될 수 있다 해도, 가용에너지의 계산에는 전문 장비 및 전문기술(예, DEXA를 통한 신체 조성 측정), 선수들의 동기 부여 및 순응(식이섭취량 기록 및 활동 일지 기록) 그리고 상당한 시간과 전문 지식 이 필요하며, 낮은 가용에너지 상태는 생리적 요구 상태가 다양하기 때문에 트레이닝 및 훈련 단계에 따라 다르게 나타날 수 있다(Mountjoy et al., 2018).
한편, 2014년에 여자 선수들의 여자 운동선수들을 위한 낮은 에너지 가용성에 대한 스크리닝 도구인 Low Energy availability in Females Questionnaire(LEAF-Q)이 개발되었다(Melin et al., 2014). 이 설문지는 78% 민감도와 90% 특이도를 보였으며, 낮은 에너지 가용성과 관련 있는 생리적 증상들의 ‘위험수준’을 확인하는데 사용될 수 있다. 이 설문지를 단독으로 사용하는 것 보다는 타당성이 증명된 이상 식이 스크리닝 도구(예, 여자 운동선수 스크리닝 도구; Female Athlete Screening Tool(FAST)과 함께 사용할 것을 권장한다. 추가적으로 최근 여자 운동선수들을 대상으로 개발된 Brief ED in Athletes Questionnaire(BEDA-Q)이 LEAF-Q와 함께 식이 장애가 있거나 없는 여자 운동선수를 식별하는데 사용될 수 있다(Logue et al., 2018).
낮은 에너지 가용성에 따른 건강 결과
1. 내분비
낮은 가용에너지가 내분비계에 미치는 영향은 주로 여자 선수들에게 나타났으나, 최근 남성 운동선수에도 나타나고 있다. 낮은 가용에너지 상태에 있는 일부 여자 선수들에게 시상하부-뇌하수체-생식선축의 장애, 갑상선 기능의 변경, 식욕 조절 호르몬의 변화(예, 렙틴 및 옥시토신 감소, 그렐린 증가, 펩티드 YY와 아디포넥틴 증가), 인슐린 감소 및 인슐린 유사 성장 호르몬 1(IGF-1), 성장 호르몬 저항 증가, 코티졸 증가와 같은 반응들이 나타났다(Allaway et al., 2016; Ihle & Loucks, 2004; Logue et al., 2018; Loucks & Thuma, 2003; Misra, 2014). 이들 호르몬 변화들은 더 중요한 신체기능을 위해 에너지를 보존하거나 생명유지를 위한 신체 에너지를 보존하기 위해 발생하는 것으로 보인다(Jasienska, 2003; Wade & Jones, 2004).
2. 생리기능
여자 운동선수들에서 낮은 가용에너지가 생리기능 및 생식 호르몬에 미치는 영향은 많이 알려져 있지만(Gordon et al., 2017; Loucks & Thuma, 2003; Nattiv et al., 2007), 이러한 영향을 뒷받침하는 복잡한 신호전달경로는 아직 완전히 밝혀져 있지 않다. 최근 낮은 가용에너지는 시상하부에서 성선 자극 호르몬 방출 호르몬(GnRH)의 불안정성(pulsatility)을 일으키고, 뇌하수체에서 황체호르몬과 난포자극호르몬 방출의 변화 및 에스트라디올, 프로게스테론 수치 감소를 가져온다는 증거가 제시되고 있으며 이것은 기능성 시상하부 무월경(functional hypothalamic amenorrhoea; FHA)의 한 형태로 여겨진다(Curry et al., 2015; Gordon et al., 2017). 이러한 체내 문제점이 얼마만큼의 기간 후 발생하는지 아직 명확하지 않으며, 연구마다 사용된 서로 다른 방법과 체내 상태의 복잡성으로 인해 이를 서로 비교하는 것은 어렵다. Loucks & Thuma(2003)은 좌식생활 양식의 여자를 대상으로 잘 통제된 실험실 연구에서 가용에너지를 30kcal/kg FFM/day 이하로 감소시켰을 때 5일간의 짧은 기간 동안 황체호르몬 변동성이 감소되는 것을 확인하였다. Williams et al.(2015)의 연구에서도 이전에 정상 월경을 하고 있는 대상자들에서 에너지 섭취 및 운동 에너지 소비 조절로 가용에너지를 감소시켰을 때 월경주기가 달라짐을 확인하였다. 그러나 에너지 부족 정도에 따라 월경장애의 빈도가 영향을 받지만, 이러한 월경 장애를 일으킬 수 있는 특정 가용에너지의 역치는 아직 불명확하다(Lieberman et al., 2018).
Reed et al.(2015)의 정상 월경 그리고 다양한 월경 상태의 여자 운동선수를 대상으로 한 단면적 연구에서 3일간의 식이 및 운동 일지 작성과 운동 중 에너지 소모량은 심박수 측정기로 모니터 하여 가용에너지를 평가하였다. 이 연구에서 모든 집단(정상월경, 희발월경, 배란성 무월경 등)은 평균 가용에너지가 30kcal/kg FFM/day 이상이었으며 가용에너지는 월경 불순의 준 임상적 형태와 관련을 보이지 않았으나, 정상 월경을 하는 선수에 비해 무월경 운동선수에서 가용에너지가 낮게 나타났다(mean 30.9 vs 36.9kcal/kg FFM/day). 심각한 에너지 부족이 무월경을 일으킨다고 잘 알려져 있지만, 짧은 기간 및 장기간의 가용에너지 부족과 월경 불순과의 관련성에 대해서는 더 많은 이해가 필요하다.
3. 뼈 건강
낮은 가용에너지가 운동선수의 뼈 건강을 감소시킨다고 알려져 있으며 이러한 관련성은 특히 여자 운동선수에서 잘 나타나고 있다. 신체적으로 활동적으로 희발월경/무월경을 겪고 있거나 낮은 가용에너지 상태의 여자운동 선수는 에너지가 충만한 정상 월경을 하고 있는 운동선수에 비해 감소된 골밀도, 뼈 미세구조 및 골 교체 마커 변화 그리고 골절에 대한 위험도가 증가하는 것으로 보고되고 있다(Ackerman et al., 2011, 2012; De Souza et al., 2008; Nattiv et al., 2007; Papageorgiou et al., 2018). 짧은 기간 동안의 낮은 가용에너지 노출도 남녀에서 골 교체 바이오마커에 부정적 영향이 나타났으며(Ihle & Loucks, 2004; Papageorgiou et al., 2017), 특정 종목의 운동선수 즉 기수, 달리기 선수 그리고 사이클 선수에서 낮은 골밀도에 대한 위험도가 증가되어 있었다(Ackerman et al., 2011, 2012; De Souza et al., 2008; Nattiv et al., 2007; Papageorgiou et al., 2018).
낮은 체질량지수는 낮은 가용에너지의 중요한 표지자이다. 체질량지수 17.5 kg/m2 이하, 청소년의 경우 예측 체중의 85% 이하, 최근 1달 동안에 10% 이상 체중 감소는 낮은 가용에너지의 지표로 제시되고 있으며(De Souza et al., 2014), 이러한 체질량지수와 체중의 임계점은 남녀 모두에서 골감소의 위험을 증가시키는 것과 관련이 있는 것으로 나타났다(Barrack et al., 2017; Tenforde et al., 2015; Thralls et al., 2016). 낮은 가용에너지는 식이장애/이상식이, 생리장애, 낮은 골밀도를 수반할 수 있으며, 뼈 손상에 대한 위험도가 높은 선수들은 이러한 요인들이 복합적으로 나타나고 있다(Ackerman et al., 2015; Barrack et al., 2014; Tenforde et al., 2017).
4. 심리적 문제
심리적 문제는 낮은 가용에너지를 유발하거나 낮은 가용에너지에 의해 심리적 문제가 발생할 수 있다(Mountjoy et al., 2014). 운동선수에서 낮은 가용에너지는 심리적 웰빙의 다양한 측면과 부정적 관련을 갖는 것으로 나타났다. 마름에 대한 갈망은 낮은 가용에너지에 대한 대리표식자가 될 수 있다. 식이장애 검사(Eating Disorder Inventory)에서 마름에 대한 갈망 점수는 여자선수들의 감소된 안정시 에너지소모량, 낮은 T3 수준, 높은 그렐린 수치와 관련을 보였으며(De Souza et al., 2007), FHA 를 가지고 있는 여자 청소년에서 가벼운 우울 성향, 정신 신체장애, 스트레스를 해소하는 능력의 감소가 더 많이 나타나는 것으로 밝혀졌다(Bomba et al., 2007; Marcus et al., 2001). 또한 신경성 거식증과 FHA를 같이 가지고 있는 청소년의 경우 건강한 청소년에 비해 우울증 및 불안감, 내성적, 체중 증가의 두려움이 높게 나타났으며, FHA 집단 보다 신경성 거식증으로 가용에너지가 제한된 집단이 더 심한 정신적 장애가 있는 것으로 나타났다(Bomba et al., 2014).
5. 이상식이 및 식이장애
이상식이와 식이장애는 체중에 민감한 스포츠 선수(남녀 모두)에서 더 잘 나타난다(Kong & Harris, 2015; Sundgot-Borgen, 1993; Sundgot-Borgen & Torstveit, 2004; Sykora et al., 1993; Thiemann et al., 2015). 노르웨이의 엘리트 청소년 남녀 선수를 대상으로 한 연구에서 설문지를 이용한 이상식이 유병률은 운동선수에 비해 비 운동선수에서 더 높게 나타났지만(Martinsen et al., 2010), 인터뷰로 평가한 결과 운동선수에서 식이장애 유병률이 더 높게 나타났다(Martinsen et al., 2013). 이러한 결과는 운동선수에서 식이 장애를 평가할 때는 개별 인터뷰가 필요하다는 점을 시사한다(Fairburn & Beglin, 2008; Martinsen & Sundgot-Borgen, 2013; SundgotBorgen & Torstveit, 2004). 식이장애의 병리 기전에는 문화, 가족, 개인 및 유전/생화학적 요소가 복합적으로 작용한다(Stice et al., 2012). 성별과 갑작스러운 훈련량 증가, 부상, 식사 장애 행동을 하는 동료, 그리고 경기 체중 측정은 체중에 대한 압박감과 독특한 식이장애 위험의 유발 요소가 된다(Arthur-Cameselle et al., 2017; Krentz & Warschburger, 2013; Sundgot-Borgen, 1994). 운동 수행력을 높이기 위한 체중 감량의 욕구는 이후 이상식이의 예측인자가 될 수 있으며(Krentz & Warschburger, 2013), 코치와 운동 선수간의 관계가 갈등이 높고 지지가 부족할 때 식이장애의 위험성이 높아질 수 있다(Shanmugam et al., 2014). 이상식이는 완벽주의, 경쟁력, 통증 내성 및 수행력에 대한 체중 감소 이점 인지에 의해 영향을 받는 것으로 보인다(Stirling & Kerr, 2012; Arthur-Cameselle et al., 2017). 따라서 체중감량을 경험한 선수, 부상당한 선수 또는 식이장애가 있는 팀원들과 함께 훈련하는 선수들에게 식이장애 선별을 통한 사전 스크리닝은 낮은 에너지 가용성 노출에 대한 예방 및 치료에 있어 중요하다고 할 수 있다. 하지만 잠재적 위험요인에 관한 인과관계가 명확하지 않기 때문에 추후 지속적인 연구가 필요하다.
낮은 에너지 가용성과 운동 수행능력
여러 연구에서 낮은 에너지 가용성의 여러 지표들(예, 호르몬 변이, 희발월경, 무월경, 체중조절 및 에너지 소비량이 많은 스포츠 참여(심미적 스포츠, 육상, 사이클 등), 이상식이/식이장애/낮은 에너지 가용성 검사 도구에서 높은 점수)과 운동수행력의 부정적 영향을 미치는 지표들(질병, 부상, 철분 부족, 감소된 인지 및 기분장애)과의 관련성이 보고되고 있다(Ackerman et al., 2015, 2019; Baskaran et al., 2017; Petkus et al., 2017). 장기간의 에너지 제한(섭취 에너지, 소비에너지)과 스포츠 경기력과의 관련성에 대한 실험연구는 부족하지만, 지속된 낮은 가용에너지가 다양한 간접적 기전(회복 감소는 신체적 정신력 능력을 조기에 감소시키고, 최적의 근육량과 근 기능 손상)을 통해 스포츠 경기력을 감소시킬 수 있다는 가설이 제시되고 있다(Fogelholm, 1994). 또한 낮은 가용에너지는 운동수행력 감소를 예측할 수 있으며, 글리코겐 저장 또는 단백질 합성과 같은 주요 과정의 일시적 감소를 통해 최적의 운동수행력 발휘를 방해 받을 수 있다(Areta et al., 2014). 또한 부상 및 질병의 위험성이 증가하기 때문에 높은 수준의 트레이닝을 못 받게 될 수도 있다(Drew et al., 2017, 2018). 에너지 가용성과 운동수행력 간에 이러한 중요한 관련성이 있음에도 불구하고 그동안 이에 관한 직접적인 연구는 매우 부족하다. 최근 엘리트 리듬 체조 선수를 대상으로 한 연구에서 에너지 가용성은 경기 순위와 관련이 있음을 보고하였으며(Vo et al., 2017), 다른 연구에서 이차성 FHA를 갖고 있는 엘리트 지구성 선수는 체중과 체지방량이 낮음에도 불구하고 무월경의 엘리트 지구성 선수와 최대산소섭취량으로 측정한 유산소성 능력은 차이가 없었으나 FHA를 갖고 있는 엘리트 지구성 선수는 정상월경 선수에 비해 근골격계 기능(하지근력 및 근지구력)와 반응 속도가 떨어져 있었다(Tornberg et al., 2017). 낮은 근골격계 수행력은 높은 코티졸 수준과 낮은 혈당, T3, 에스트로겐과 측정 다리에서 낮은 제지방량과 관련을 보였다. 비록 단위 질량 당 더 강한 힘이 달리기 수행력에서 중요하다고 여겨지지만, 이 연구에서 지속적인 에너지 제한으로 이상적인 체중과 체성분을 만든다면 이는 오히려 건강과 운동수행력에 부정적인 영향을 미칠 수 있다고 경고하고 있다(Tornberg et al., 2017). 남녀 국가대표 조정팀을 분석한 Woods et al.(2017)의 연구에서도 4주간의 강화 훈련 기간 동안 트레이닝량은 21%가 증가함에도 불구하고 에너지 섭취량은 부족하였으며, 이러한 부적절한 에너지 가용성은 트레이닝 후 회복에 부정적 영향을 미쳤다고 제시하였다. 또한 Vanheest et al.(2014)은 12주 간의 트레이닝 기간 후 400m 시간 시험에서 수영 속도가 정상월경의 팀원들은 8% 수행력이 증가한 반면 에너지 부족에 따른 난소 억제를 가진 젊은 엘리트 수영 선수는 오히려 약 10% 감소하였다고 보고하였다. 훈련적응과 운동 수행력에 대한 낮은 에너지 가용성의 더 많은 증거 및 설명력을 높이기 위해 운동선수들을 대상으로 한 더 많은 조사가 필요하다.
RED-S의 예방
RED-S를 예방하려면 무엇보다도 운동선수와 관계자(지도자, 부모 등)의 인식을 높여야 한다. 설문 조사에 따르면 의사, 코치, 물리 치료사 및 운동 트레이너의 50% 미만이 Triad 구성 요소(섭식 장애, 월경 기능 장애 및 낮은 BMD가 있거나 없는 LEA)를 식별할 수 있다고 보고하였다(Brown et al., 2014; Curry et al., 2015; Feldmann et al., 2011; Kroshus et al., 2014; Mukherjee et al., 2016; Pantano, 2006; Troy et al., 2006), 또한 370명의 미국 고등학교 간호사 중 19%만이 식별할 수 있었다. 세 가지 Triad 구성 요소 모두(Kroshus et al., 2015) 931명의 다분야 전문의를 대상으로 한 설문조사에서 37%만이 Triad를 알고 있었고 이 중 1/2만이 환자를 편안하게 치료하거나 의뢰할 수 있었다(Curry et al., 2015). 운동을 하는 호주 여성 그룹에서 3분의 1은 불규칙한 생리가 활동적인 여성에게 “정상”이라고 믿었으며 대략적으로 절반은 월경 장애가 뼈 건강 악화의 위험 요소라는 것을 알고 있었다(Miller et al., 2012). 우리나라의 경우도 국가대표 여자선 총 76명을 대상으로 여자선수 3징후에 관한 인식도를 조사한 결과 91%가 모르고 있었으며, 알고있다고 답한 9% 선수들도 구성요소에 대하여는 정확히 알고 있는 사람이 단 한 명도 없었으며(Park, 2020), 242명의 엘리트 여자선수들에게서 RED-S에 대한 인식도를 조사한 결과 95%는 모른다 라고 답하였고, 5%만이 알고 있다고 답하였다(Park, 2021). 이런 근거는 RED-S에 대한 이해를 높이는 것이 필요하다는 것을 말해주고 있다.
선행 연구를 살펴보면, 여성 운동선수를 위한 교육프로그램 중재를 통해 1년 동안 폭식증을 개선하였으며(Becker et al., 2012), 엘리트 남성 및 여성 운동선수(Martinsen et al., 2014)와 코치(Martinsen et al., 2015)를 포함하는 노르웨이 학교 기반 통제 중재 프로그램은 중재 학교에서 여성 사이에서 새로운 섭식 장애 사례를 초래하지 않았으나 통제군 학교의 여학생은 8명(13%)으로 증가하였다(Martinsen et al., 2014). 이러한 결과는 효과적인 섭식장애 및 섭식장애 예방을 위해서는 운동선수 및 코치 이외에 개인, 성별에 따른 이 운동선수 및 코치 이외의 개인을 대상으로 하고, 성별에 따른 예방 교육이 필요하며, 뿐만 아니라 의료 시스템, 스포츠 규정의 변경, 정책 조치가 포함되는 것이 중요하다(De Bruin, 2017)라 할 수 있다.
RED-S를 위한 스크리닝
RED-S는 관련 요인 즉, 가용에너지 수준, 식이장애 유무, 월경기능, 뼈 건강 상태 검진을 통해 진단될 수 있다. 정확한 진단은 의료진을 통해 이루어질 수 있으나, RED-S는 조기 진단 및 예방이 매우 중요하므로 선수 스스로 자신의 건강 상태 및 관련 증상들을 모니터 할 수 있어야 한다. 이에 미국 스포츠의학회에서는 여자운동선수 3징후와 관련된 증상들을 선수 스스로가 스크리닝 해 볼 수 있는 참가 전 자가진단 질문(preparticipation physical evaluation; PPE)을 매년 건강 평가 시 체크하도록 권고하고 있다(De Souza et al., 2014). IOC에서도 운동선수들의 스포츠 참가 허용 및 부상 후 회복을 결정하기 위한 진단적 도구로 RED-S Clinical assessment tool(RED-S CAT)를 개발하였으며(Mountjoy et al., 2015), 전반적인 가용에너지 감소에 인해 나타날 수 있는 운동 중 부상 및 생리기능 장애, 위장기능 장애를 평가할 수 있는 LEAF-Q 등 다양한 자가진단 도구들이 사용되어 오고 있다(Tayne et al., 2019). 본 종설에서는 선행연구를 참고하여 선수들이 보다 쉽고 간단하게 RED-S 위험성을 스스로 평가할 수 있도록 아래[그림 3]과 같이 도식도 형태로 재구성하였다(Park, 2020). 월경장애, 식이장애 그리고 운동 중 부상이력에 대해 묻는 각 질문은 모두 ‘O/X’의 형식으로 답할 수 있으며 답에 대한 도식을 따라 현재 상태를 자가 진단 할 수 있다. ‘만 15세까지 초경 경험이 없거나 정상 월경을 하지 않는 경우, 낮은 골밀도에 대한 진단을 받은 경우, 혹은 거식증을 앓고 있는 경우’ 이 질문들 중 한 가지라도 해당이 된다면 전문 의료진의 상담 및 진료를 받아야 한다. 또한 최근 3개월 이내 부상이력이 있는 경우 골밀도에 대한 가족력과 과거의 장골 골절 이력 여부에 따라 추가적인 검사를 받아야 한다. 가족력이나 골절이력이 없더라도 가용에너지 검사(LEAF-Q)를 실시하여 낮은 가용에너지에 대한 평가를 진행하고 앞으로의 부상을 예방을 위해 RED-S 예방 및 치료 지침을 지켜야 한다. 또한 현재 저체중이거나 체중에 대한 강박이 있는 경우도 가용에너지 검사 후 RED-S 예방 및 치료 지침을 따를 것을 권한다.
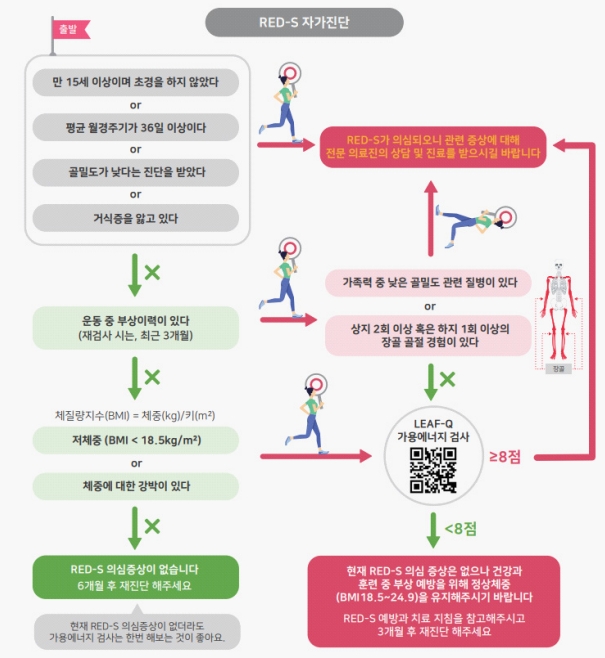
Algorithm for RED-S screening
정확한 상담 및 진료를 위해 경험이 많은 의료팀(의사, 스포츠과학자, 트레이너, 컨설턴트 등)을 구성한 후, 의사 주관 하에 각 분야 전문가들의 의견을 수렴하여 섭식장애, 월경장애 골감소증에 대한 각각의 증상을 진단해야 한다(De Souza et al., 2014).
결론 및 제언
여자선수들의 섭식장애 또는 낮은 에너지 가용성(Low Energy Availability; LEA), 생리 기능장애(무월경), 낮은 골밀도의 유병률은 일반 여자들에 비해 높은 것으로 나타났다(Sundgot-Borgen & Torstveit, 2004), 그 중 LEA는 부족한 에너지 섭취량 혹은 과도한 훈련량으로 인해 나타나는 상대적 에너지 부족의 결과로써 나타나는 건강결과와 운동수행력을 저하시키는 대리표시자(surrogate marker)라 할 수 있다(Ackerman et al., 2019). 이에 많은 연구자들은 여자선수들의 특이적 지원 시스템을 통해 선수의 경기력 향상 및 삶의 질을 높이고자 노력하고 있으며, 특히 선수, 지도자, 부모에게 RED-S와 관련된 다양한 증상으로 인한 문제점을 인지할 수 있는 교육 프로그램 개발에 대한 중요성을 제시하고 있다.마지막으로 여자 선수의 RED-S의 발병은 일시적일 뿐만 아니라 은퇴 후 건강한 삶을 방해하는 요인으로 작용하기 때문에 무엇보다 예방이 중요하다.