가쪽 발목 염좌 병력 여부에 따른 유소년 운동선수의 동적 자세 제어 비교
Comparison of Dynamic Postural Control in Youth Athletes with and without a History of Lateral Ankle Sprain : A Case-control Study
Article information
Abstract
[목적]
본 연구의 목적은 유소년 운동선수의 발목염좌 경험 여부에 따른 동적 자세 조절 능력 차이를 관찰하는데 있다.
[방법]
28명(발목손상 집단 14명, 건강한 집단 14명)의 유소년 운동선수가 본 연구에 참여하였다. 모든 대상자는 주관적 발목 불안정성 평가 설문지를 작성하였고, 동적자세조절 능력 평가인 Star Excursion Balance Test (SEBT)에 참여하여 하지관절각, 압력중심점(center of pressure, COP) 범위 및 속도를 수집하였다. 통계처리는 각 변인의 집단 간 차이를 분석하기 위해 정규성 검정에 따라 독립표본 t 검정 또는 Mann-Whitney U 검정을 실시하였다.
[결과]
발목손상 집단(LAS)은 스포츠 참여 경력이 건강한 집단(CON)에 비해 오래되었고 주관적 발목 불안정성 평가 점수가 낮게 관찰되었다(p<0.05). LAS는 CON에 비해 SEBT의 앞쪽에서 짧은 도달 거리, 적은 엉덩관절 굽힘 및 발등굽힘 각도가 관찰되었다(p<0.05). 또한, LAS는 CON보다 SEBT의 뒤안쪽에서 앞-뒤 및 가-안쪽 COP 속도가 더 느렸고, SEBT의 뒤가쪽에서 앞-뒤 COP 속도가 더 느리게 나타났다(p<0.05). 그 외 다른 변인에서는 그룹 간에 차이가 없었다(p>0.05).
[결론]
본 연구의 결과를 기반으로 SEBT 앞쪽 수행 시 LAS는 시상면에서 하지 관절의 동적 자세 제어 전략을 변경함으로써 도달 거리를 감소시키는 것으로 확인되었다.
Trans Abstract
PURPOSE
The purpose of this study was to compare the dynamic postural control of youth athletes with and without a history of lateral ankle sprains.
METHODS
Twenty-eight youth athletes (14 lateral ankle sprain, 14 healthy control) participated in this study. All participants answered the Foot and Ankle Ability Measure questionnaire and were subject to the Star Excursion Balance Test (SEBT) for dynamic postural control evaluation to collect the joint angles of the lower extremity, a center of pressure (COP) path, and COP velocity. Independent sample t-test or Mann-Whitney U-test were performed to analyze the difference between the groups.
RESULTS
The lateral ankle sprain group (LAS) was found to have a long experience in participating in sports, and low Foot and Ankle Ability Measure scores were identified when compared to the healthy control (CON; p<0.05). LAS was observed with a short reach distance, less hip flexion, and dorsiflexion angles during the anterior direction of SEBT when compared to CON (p<0.05). Furthermore, LAS showed a slower anteroposterior and mediolateral center of pressure velocities in the posteromedial aspect of SEBT and a slower anteroposterior COP velocity in the posterolateral aspect of SEBT when compared to that of CON (p<0.05). There were no differences between the groups with respect to the other variables (p>0.05).
CONCLUSIONS
Based on these results, decreased anterior reach distance of SEBT may be affected by changing the dynamic posture control strategy of the lower extremity joint on the sagittal plane in LAS.
서론
생물학적 및 인지 발달이 나타나는 유소년기에 체계적이고 전문화된 스포츠 훈련에 참여한 선수는 상대적으로 늦은 나이에 시작한 선수보다 원하는 기술을 빨리 배우고, 우수한 수준의 기술을 구사하는 것으로 보고된다(Ericsson et al., 1993). 그러나 유소년기는 비선형적인 급성장이 나타나는 시기로 일시적인 감각운동 기능 지연으로 인해 자세제어의 어려움이 발생하며 이는 근골격계 손상의 위험요인으로 작용한다(John et al., 2019; Quatman-Yates et al., 2012). 근골격계 부상은 동적 자세제어에 요구되는 시각, 체성감각, 전정감각기관 중 관절의 움직임 및 위치에 대한 정보를 제공하는 체성감각의 결함이 관찰되며, 이는 새로운 근골격계 부상 또는 재부상의 위험을 증가시킬 수 있다(Baker et al., 2009; Dalton, 1992; Gribble et al., 2012; Van Der Sluis et al., 2014).
유소년기 운동선수의 대표적인 부상부위는 발목관절이며(Korea Sports Safety Foundation, 2020; Lambers et al., 2012), 그 중 48.9%는 충돌, 무리한 동작, 넘어짐, 점프 후 착지 오류 등에 의해 발생하는 염좌(sprain)의 형태로 보고된다(Ha et al., 2021; Korea Sports Safety Foundation, 2020). 발목염좌는 구조적, 기능적 결함을 유발하는데 손상 정도에 따른 적절한 치료가 제공되지 않는다면 만성 발목 불안정성(chronic ankle instability)으로 발전하여 스포츠 기술 수행능력의 저하, 참여시간의 감소 및 중단이 나타날 수 있다(Cloke et al., 2011; Ha et al., 2021; Hubbard-Turner, 2019; Mandarakas et al., 2014; Roos et al., 2017). 성인 운동선수와 유소년 운동선수의 발목염좌 발생률은 차이가 없으나 만성발목불안정성의 발생률은 유소년이 성인에 비해 높은 것으로 보고된다(Tanen et al., 2014). 유소년기의 발목불안정성 발생은 성인보다 긴 시간 발목기능부전과 재부상위험에 노출시킨다(Konradsen et al., 2002; Marchi et al., 1999; Weir & Watson, 1996). 따라서 유소년기 운동선수들의 발목염좌 발생 후 동적 자세제어 전략을 이해하는 것은 근골격계 부상 없이 성인 운동선수로 성장하는데 도움이 될 것이다.
발목염좌 발생 이후 걷기, 달리기 등 다양한 활동에서 관절 움직임의 차이가 나타난다. 발목염좌 과거력이 있는 경우 걷기 시 발꿈치 딛기(heel strike) 앞뒤로 앞발의 안쪽번짐 관절각과 모멘트의 크기가 과거력이 없는 경우보다 크게 나타났고(Monaghan et al., 2006), 조깅 시 발목염좌 과거력이 있는 경우 발등굽힘 가동범위의 결측이 보고되었다(Drewes et al., 2009). 발목염좌에 따른 관절 움직임의 차이가 보고되나 대부분의 연구는 성인을 대상으로 실시되어 유소년의 동작변화를 이해하는데 어려움이 따른다.
동적 자세제어는 외부에서 가해지는 자극 또는 자발적인 움직임 동안 넘어지지 않는 능력을 의미한다. 이를 평가하기 위해 사용하는 Star Excursion Balance Test(SEBT)는 하지 근력, 균형성, 협응력, 유연성을 복합적으로 요구하는 동작으로 구성되어 있는 저렴하고 측정시간이 짧은 도구이다(Plisky et al., 2006). 국내 스포츠 현장 및 현장 중심연구에서 SEBT는 발목염좌 병력이 있는 중등부 축구선수와 병력이 없는 대조군간의 신체 능력 및 특성의 변화 차이 분석(Lee et al., 2021), 플라이오메트릭과 코어강화 훈련 효과 분석(Jo & Choi, 2018), 키네시오 테이핑 적용의 유효성 분석(Cho et al., 2021) 등 다양한 연구목적 하에 사용되고 있다. 정량적 평가를 위해 도달거리를 다리길이로 표준화한 값으로 나타내고 있으나 어떤 전략의 변화로 표준화된 도달길이의 차이가 나타난 것인지에 대한 설명이 어렵다는 단점이 있다. 따라서 SEBT 도구의 효율적인 사용을 위해 운동학적 변화 요인을 이해하기 위한 분석이 필요한 실정이다. 본 연구의 목적은 유소년 운동선수의 발목염좌 경험 여부에 따른 동적 자세 조절 능력 차이를 관찰하는데 있다.
연구방법
연구대상
배구, 축구, 필드하키, 핸드볼 종목 유소년 운동선수 중 발목손상 과거력이 있는 14명(배구=4명, 축구=6명, 핸드볼=4명)과 하지손상 과거력이 없는 14명(배구=1명, 축구=3명, 필드하키=9명, 핸드볼=1명)의 선수가 본 연구에 참여하였다(Table 1). 연구대상자의 선정기준은 다음과 같다: 발목손상 집단은 가쪽 발목 염좌(lateral ankle sprain) 외 다른 하지부상 경험이 없는 자; 건강한 집단은 근골격계 부상 경험이 없는 자. 두 집단 공통기준으로 1) 최근 3개월 내 근골격계 부상이 없으며, 2) 전문운동선수로 각 협회에 등록된 자, 3) 훈련과 경기에 참여하고 있는 자로 선정하였다. 본 연구는 연구기관 내 생명윤리위원회의 승인을 받은 후 진행되었으며(KISS-21018-2111-04), 대상자의 자발적 동의 후 실행하였다.
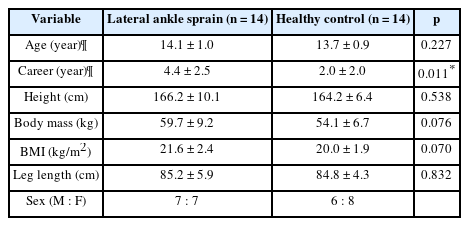
Demographic characteristics of participants
연구절차
모든 대상자는 키, 몸무게, 다리길이(체중이 지지된 상태에서 위앞엉덩뼈가시부터 안쪽복사뼈까지의 길이) 측정 후 주관적 발목 불안정성 평가 설문지(Foot and Ankle Ability Measure, FAAM)와 SEBT에 참여하였다.
FAAM은 두 개 항목으로 구성되어 일상 생활 활동(activities of daily, ADL)과 스포츠 활동(sports) 중 주관적 발목 불안정성을 평가하는 도구이다. 각각 21개, 7개의 문항으로 구성되며, 5점 척도로 평가된다: 4점, 어려움 없음; 3점, 약간의 어려움; 2점, 보통 수준의 어려움; 1점, 극심한 어려움; 0점, 활동 불가(Ha, 2015).
SEBT는 만성 발목 불안정성과 관련된 기능적 결함을 찾고 (Doherty et al., 2016), 하지 부상 위험요인을 갖은 선수를 선별하며(Nagamoto et al., 2021), 발목부상 후 회복정도를 평가하는 도구이다(Doherty et al., 2015). SEBT는 3차원 동작분석 장비를 사용하여 평가하였다. 모든 대상자는 상·하의 타이즈를 착용하고 하체에 마커(marker) 30개를 부착하였다. 하체를 7개의 분절로 모델링하기 위하여 양쪽 위앞엉덩뼈가시, 양쪽 엉덩뼈가시, 양쪽 위뒤엉덩뼈가시, 양쪽 큰돌기, 양쪽 넙다리, 양쪽 뒤넙다리, 양쪽 무릎 가쪽 위관절융기, 양쪽 무릎 안쪽 위관절융기, 양쪽 정강이뼈거친면, 양쪽 가쪽 복사, 양쪽 안쪽 복사, 양쪽 첫 번째 발허리뼈머리, 양쪽 다섯 번째 발허리뼈머리, 양쪽 발가락, 양쪽 발꿈치뼈에 마커를 부착하였다. 모든 대상자는 연구자에게 평가 방법에 대한 설명을 듣고, 준비운동과 연습 시간을 제공받았다. 대상자는 개인 운동화를 착용하고 바닥에 그려진 선의 중앙에 외발로 균형을 잡고 서도록 요청받았다. 발목손상 집단은 발목손상 경험이 있는 발을 측정하였고, 건강한 집단은 주동발을 측정하였다. 앞쪽(anterior), 뒤안쪽(posteromedial), 뒤가쪽(posterolateral) 방향으로 <Figure 1>과 같이 양 손은 허리에 고정하고 공중에 있는 발을 최대한 뻗어 바닥을 가볍게 찍고 오는 것을 3회씩 반복측정 하였다. 만약 동작수행 중 대상자가 1) 균형을 잃고 넘어지거나 2) 발이 지면에서 떨어지거나 3) 허리에 고정한 손이 떨어지거나 4) 공중에 있는 발이 바닥을 찍지 못한 경우 실패로 간주하고 추가로 측정하였다.

Star excursion balance test for the (A) anterior, (B) posteromedial, (C) posterolateral reach directions
자료처리
FAAM-ADL과 FAAM-sports는 84점 만점에서 각 문항에서 합산된 점수의 차를 통해 백분율로 산출하였다. 백분율이 낮을수록 주관적 발목 불안정성이 높음을 의미하고, FAAM-ADL 90%미만, FAAM-sports 80%미만은 만성 발목 불안정성으로 평가할 수 있다.
운동역학적 분석을 위해 지면반력기(Kistler, Sweden) 1대, 운동학적 분석을 위해 Oqus700+ 적외선 카메라(Qualisys, Sweden) 20대를 사용하였다. 각각의 샘플링율은 2500Hz, 250Hz로 설정하였다. 획득된 자료는 Visual 3D(C-motion, USA)를 이용하여 노이즈 제거를 위해 차단주파수 6Hz로 Butterworth Bidirectional low-pass filter를 수행하였다. 발목, 무릎, 엉덩관절의 3차원 각도는 최대 거리에 도달한 시점을 분석하였고, 압력중심점의 앞–뒤, 가–안쪽 경로 및 속도는 준비자세에서 최대 거리에 도달한 시점까지의 구간을 분석하였다. 각정의는 다음과 같다: 엉덩관절, 굽힘(+)/폄(–), 벌림(+)/모음(–), 가쪽돌림(+)/안쪽돌림(–); 무릎관절, 굽힘(+)/폄(–), 밖굽이(+)/안굽이(–), 가쪽돌림(+)/안쪽돌림(–); 발목관절, 발등굽힘(+)/발바닥굽힘(–), 가쪽번짐(+)/안쪽번짐(–), 가쪽돌림(+)/안쪽돌림(–). 또한, 스포츠 현장에서 사용하는 분석 지표인 지지하고 있는 발과 공중에서 각 방향으로 최대한 뻗어 바닥에 접촉한 위치까지의 거리를 제시하였다. 마커 기반으로 발분절의 중심부터 발가락 마커 간 거리(reaching distance)를 산출하였고, 각 방향 최대 거리는 다리 길이(leg length, LL)로 표준화한 후 백분율로 표기하였다. SEBT 종합점수(composite score)는 세 방향의 도달거리의 합을 다리길이 3배수로 나누어 백분율로 표기하였다.
통계분석
연구목적에 따라 가쪽 발목 염좌 경험이 있는 집단의 주관적 발목 불안정성 결과, 동적 자세 조절 능력 평가 결과 차이를 비교하기 위해 정규성 검정에 따라 독립표본 t-검정과 Mann-Whitney U-검정을 통해 분석하였고, 효과크기 Hedges’ g와 95% CI(confidence interval)를 산출하였다: 0.2≤Small effect<0.5; 0.5≤Medium effect<0.8; Large effect≥0.8. 통계적 유의수준은 α=0.05로 설정하였으며, 분석프로그램은 SPSS 25.0(IBM, USA)을 사용하였다.
연구결과
발목손상 집단은 건강한 집단 보다 선수 경력이 길게 관찰되었으나(Z=–2.514, p<0.05), 나이, 키, 몸무게, 체질량지수, 다리길이에서는 통계적 차이가 나타나지 않았다(p>0.05; Table 1).
주관적 발목 불안정성 평가 결과 하위항목 인 FAAM-ADL(발목손상 집단 92.01±14.36%, 건강한 집단 100.00±0.00%; Z=4.029, p<0.001)과 FAAM-Sports(발목손상 집단 84.19±19.19%, 건강한 집단 100.00±0.00%; Z=4.018, p<0.001)에서 각각 통계적으로 유의한 차이가 관찰되었다.
SEBT-앞쪽 수행 시 발목손상 집단이 건강한 집단보다 엉덩굽힘각(t=–2.329, p<0.05)과 발등굽힘각(t=–3.009, p<0.01)이 각각 작게 나타났다(Table 2). SEBT-뒤안쪽 수행 시 발목손상 집단이 건강한 집단보다 압력중심점(center of pressure, COP)의 앞-뒤(t=–2.646, p<0.05), 가-안쪽(t=2.076, p<0.05) 속도에서 각각 느리게 관찰되었다(Table 3). SEBT-뒤가쪽 수행 시 발목손상 집단의 COP 앞-뒤쪽 속도가 건강한 집단보다 느리게 나타났다(t=–2.548, p<0.05; Table 4). 그 외 각 방향에서의 관절각과 COP 변인에서 통계적 차이가 나타나지 않았다(p>0.05; Table 2-4). SEBT 도달거리는 앞쪽으로 수행 시 발목손상 집단(75.65±7.75%LL)과 건강한 집단(82.50±5.44%LL)에서 통계적 차이가 관찰되었고(t =–2.705, p<0.05; Hedges’ g=–0.99, 95% CI=–1.81 to –0.22), 뒤안쪽(발목손상 집단 71.78±14.44%LL, 건강한 집단 72.26±11.38%LL; t=–0.099, p=0.922; Hedges’ g=–0.04, 95% CI=–0.78 to 0.70), 뒤가쪽(발목손상 집단 82.32±14.61%LL, 건강한 집단 87.16±9.08%LL; t=–1.504, p=0.303; Hedges’ g=–0.39, 95% CI=–1.14 to 0.35) 방향과 종합점수(발목손상 집단 76.58±11.18%LL, 건강한 집단 80.64±7.24%LL; t=–1.414, p=0.266; Hedges’ g=–0.42, 95% CI=–1.18 to 0.32)에서는 통계적 차이가 나타나지 않았다(Figure 2).
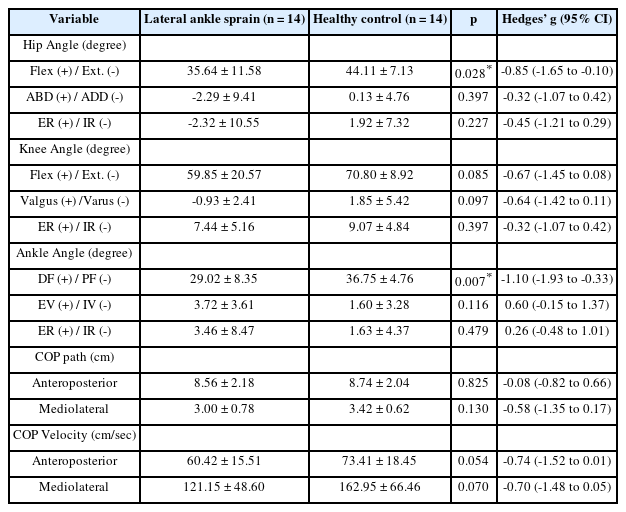
Comparison of joint angle and COP variables of the standing leg between groups at reaching anterior direction of the SEBT

Comparison of joint angle and COP variables of the standing leg between groups at reaching posteromedial direction of the SEBT

Comparison of joint angle and COP variables of the standing leg between groups at reaching posterolateral direction of the SEBT

Comparison of the results of the Star Excursion Balance Test between groups. Abbreviation: LL, leg length
논의
본 연구를 통해 유소년 운동선수의 발목염좌 경험에 따른 동적 자세 조절 차이를 확인하였다. 발목염좌 집단은 건강한 집단과 비교해 나이, 키, 몸무게, 체질량지수, 다리길이에서 통계적 차이가 없었으나 운동경력에서 통계적 차이가 관찰되었다. Ha et al.(2021)은 13-18세 전문체육인 발목염좌의 86%가 중·고급자에서 발생한 것으로 보고하였다. 엘리트 스포츠는 건강증진을 목적으로 하는 생활스포츠와 달리 경쟁의 요소가 강화되어 있어 몸싸움과 무리한 동작이 빈번히 발생한다. 고급자의 비중이 높은 19-29세 전문체육인에서는 더 높은 비중으로 몸싸움과 무리한 동작으로 인한 발목손상이 나타나는 것으로 보고되었다(Ha et al., 2021). 비록 초보자가 중·고급자 보다 심각한 손상을 입는 경우가 많다고 하지만 가벼운 손상도 반복된 다면 더 큰 손상을 야기할 수 있으므로 철저한 사후관리가 요구된다(Peterson et al., 2000). 또한 유소년 선수들의 경우 부상의 노출은 성장에 영향을 미칠 수 있으므로 급성장한 신체에 적응하는 훈련뿐만 아니라 발목 부상예방을 위한 훈련이 필수적으로 적용되어야 한다.
주관적 발목 불안정성 평가에서 발목염좌 집단은 건강한 집단보다 낮은 점수가 관찰되었으나 발목불안정성으로 분류하기에 높은 점수에 해당한다. 근골격계 부상을 경험한 은퇴선수가 자각하는 발목불안정성 점수는 FAAM-ADL 92.8%, FAAM-Sport 84.6%로 본 연구 결과와 비슷한 수준으로 나타났다(Lee et al., 2020). 이는 건강관련 삶의 질뿐만 아니라 하지의 전반적인 기능과 관련이 있는 것으로 보고되었다(Lee et al., 2020). 따라서 발목염좌 후 주관적인 발목 불안정성 개선을 위한 기능적, 심리적 중재(intervention)가 요구된다.
본 연구결과 SEBT-앞쪽의 표준화된 도달거리는 발목손상 집단이 건강한 집단보다 짧게 관찰되었다. 발목염좌 병력이 있는 유소년 축구선수에서도 본 연구결과와 같이 SEBT-앞쪽 수행 시 거리 결측을 보고하였다(Nagamoto et al., 2021). SEBT 수행 중 도달거리에 영향을 미치는 운동학적요인을 분석한 선행연구에 의하면 엉덩관절 및 무릎관절의 굽힘각으로 78% 설명할 수 있다고 하였다(Robinson & Gribble, 2008). 본 연구에서 발목염좌 집단이 건강한 집단보다 엉덩굽힘각과 발등굽힘각이 유의하게 작게 관찰되었고, 무릎굽힘각은 통계적으로 유의하지 않지만 중간 효과크기가 관찰되었다. 발목염좌 경험은 동적 자세제어 시 발목관절 뿐만 아니라 무릎과 엉덩관절의 시상면 움직임 결측이 나타남을 알 수 있다. 우리나라 유소년 전문체육인의 경우 발목염좌 발생 시 스포츠의학전문가를 통해 문제를 해결하는 비율이 약 54%에 해당하고 46%는 자가치료를 통해 처치하는 것으로 보고되었다(Ha et al., 2021). 다른 관절 손상에 비해 가볍게 생각하는 경향으로 부적절한 치료와 재활의 후유증으로 생각되며, 이는 만성 발목 불안성의 위험요인으로 작용할 것으로 사료된다(Hoch et al., 2012; Hubbard-Turner, 2019; Jaber et al., 2018).
SEBT-앞쪽과 달리 본 연구결과 SEBT-뒤안쪽, 뒤가쪽의 표준화된 도달거리는 각각 발목염좌 집단과 건강한 집단간 차이가 나타나지 않았다. 또한, SEBT-뒤안쪽, 뒤가쪽 수행 시 집단간 하지 관절의 운동학적 차이가 각각 관찰되지 않았다. 체계적 문헌고찰 및 메타분석 연구결과에 의하면 만성 발목 불안정성이 있는 자가 건강한 자보다 앞쪽, 뒤안쪽, 뒤가쪽의 짧은 도달거리를 나타내며 균형능력이 나쁜 것으로 보고하였다(Song et al., 2022). 본 연구의 대상자는 선행연구와 달리 FAAM-ADL, FAAM-Sports점수를 통해 알 수 있듯이 만성 발목 불안성 기준인 80%, 60%보다 높아 동적 자세제어 기능이 나은 것으로 생각된다. 또한 발목 불안정성은 SEBT-뒤안쪽과 뒤가쪽이 SEBT-앞쪽보다 수행능력이 먼저 개선되는 것으로 중재 연구에서 보고된다(Hale et al., 2007; McKeon et al., 2008). 이와 같은 이유로 본 연구의 발목손상 집단 대상자들은 손상 후 시간이 지남에 따라 동적 자세 제어 능력의 일부분이 개선된 것으로 판단된다. 그러나 스포츠에 참여하고 있는 현 시점에도 여전히 온전한 동적 자세 제어의 결함이 남아있어 부상의 위험요인을 갖고 있는 것으로 생각된다.
SEBT 수행 시 COP 속도변인에서 모두 0.7 이상의 효과크기를 나타냈으며 발목염좌 집단이 건강한 집단보다 SEBT-뒤안쪽 수행 시 앞-뒤, 가-안쪽, SEBT-뒤가쪽 수행 시 앞-뒤쪽의 COP속도는 통계적으로 유의한 차이가 나타났다. 두 방향에서 집단간 도달거리 및 하지관절의 운동학적 변인, COP 범위는 차이가 나타나지 않았으나 COP 속도가 느리게 나타났다. Gribble & Hertel(2004)은 자세 제어 시 피로의 발생은 발목에서 보상적 수축을 감소시켜 관절의 위치를 유지하고 COP 속도를 최소화한다고 보고하였다. 발목염좌의 경험은 선행연구의 피로 유발과 같이 원심성(efferent) 통제의 결함으로 작용하여 자세제어를 위한 발목관절의 보상수축의 어려움으로 나타난 것으로 생각된다. 본 연구 결과를 바탕으로 발목염좌 집단은 COP 속도 감소를 통해 발목관절의 움직임을 최소화하는 전략으로 동적움직임을 수행하는 것으로 사료된다. 중재에 이러한 특징을 반영한다면 환경조건의 경우의 수를 늘려 다양한 자극을 제공함으로써 재손상을 예방할 수 있을 것이다. 또한, 스포츠 현장에서 동적 자세 제어 능력을 평가하거나 발목손상 집단이 건강한 집단만큼 회복된 것을 확인하기 위해 SEBT 도달거리만으로 평가하기보다 주관적 발목 불안정성 또는 이동이 가능한 압력센서를 사용하여 COP 범위 및 속도 차이 확인이 필요할 것으로 생각된다.
결론 및 제언
본 연구를 통해 유소년 운동선수의 발목염좌 경험은 SEBT-앞쪽으로 동작 수행 시 시상면에서 하지관절의 동적 자세 조절 전략을 변화시켜 도달거리의 감소시키는 것으로 확인되었다. 발목염좌 후 동적 자세 제어의 회복을 평가하기 위해서는 SEBT-앞쪽이 유용한 지표가 될 수 있을 것이다. 또한, 발목염좌 후 하지관절의 시상면에서의 움직임 개선은 부상의 위험요인을 감소시킬 수 있을 것으로 생각된다.
본 연구는 몇몇 제한점이 존재한다. 첫 번째, 대상자의 성숙정도 및 성장도를 고려하지 못했다. 선행연구에 의하면 생물학적 성숙정도가 정적 및 동적 자세 조절에 영향을 미치는 것으로 나타났다(John et al., 2019). 두 번째, 표본크기가 상대적으로 적었다. 추후 연구에서는 본 연구의 제한점을 보완하여 성숙정도에 따른 유소년의 발목염좌 경험에 따른 동적 자세 제어 차이를 분석할 필요가 있다.
Notes
CONFLICT OF INTEREST
논문 작성에 있어서 어떠한 조직으로부터 재정을 포함한 일체의 지원을 받지 않았으며 논문에 영향을 미칠 수 있는 어떠한 관계도 없음을 밝힌다.
AUTHOR CONTRIBUTION
Conceptualization: S Ha, J-N Kim; Data curation: S Ha, J-NKim; Formal analysis: S Ha; Funding acquisition: J-N Kim; Methodology: S Ha, J-N Kim; Project administration: J-N Kim; Visualization: S Ha; Writing-original draft: S Ha; Writing-review & editing: J-N Kim