운동 후 심박회복에 따른 자율신경계의 경시적 조절: 팔과 다리의 국소적인 비교
Autonomic Nerve Regulation After Arm- or Leg Ergometer Exercising Eliciting the same heart rate level
Article information
Abstract
본 연구는 상·하지의 국소적 신체부위를 이용한 일회성 유산소 운동의 post-exercise recovery(REC)에서 나타나는 심박변이도(heart rate variability, HRV)의 차이를 살펴봄으로써 자율신경 향상을 위한 효율적 운동모드를 탐색하기 위한 목적으로 수행되었다. 건강한 젊은 남성 11명을 대상으로 무작위교차설계를 통해 동일한 강도의 여유심박수(50% heart rate reserve) 하에서 30분 간 Arm ergometer(AE) 및 Leg cycling(LE)의 평형상태운동(steady state exercise) 후 REC1(0~10 min), REC2(10~20 min), REC3(20~30 min)의 세 구간에서 R-R intervals를 획득하여 시간 및 주파수와 비선형지수(Poincaré plot)를 산출하였다. 결과는 다음과 같다. HRV의 시간영역지수를 이용해 운동모드 간의 차이를 평가한 결과 post-exercise recovery에서 AE 수행 후에 비해 LE 수행 후 ANS 조절능(SDNN) 및 PNS 재활성화(rMSSD)가 높게 나타났다. Poincare plot을 이용해 운동모드 간의 차이를 분석한 결과 post-exercise recovery에서 AE 수행 후에 비해 LE 수행 후 ANS 조절능(SD2) 및 PNS 재활성화(SD1)를 반영하는 HRV parameters의 회복률이 높게 나타났다. Spectral power 분석에서 부교감신경 재활성화를 독립적으로 반영하는 HF가 초기 post-exercise recovery(REC1)에서 AE 수행 후에 비해 LE 수행 후 유의하게 증가하였으며, 교감-미주신경 밸런스(sympathetic-vagal balance)의 교감신경 활성화를 반영하는 지수인 LF/HF ratio 와 LF nu는 AE 수행 후 유의하게 높은 수치를 나타낸 반면 부교감신경 활성화를 반영하는 지수인 HF/TP ratio와 HF nu는 LE 수행 후 유의하게 높은 수치를 나타내었다. 이상의 결과는 심박수를 일치시킨 다리의 국소적 운동이 팔의 국소적 운동에 비해 운동 후 부교감신경 재활성화가 신속하게 나타난다는 것을 암시한다. 따라서 상지에 비해 하지를 이용한 유산소 운동은 운동 후 부교감 재활성화 및 교감 활동의 빠른 억제를 통해 자율신경계의 조절에 긍정적인 영향을 미치며, 운동 후 자율신경회복이 심장사고(events)와 관련한다는 점에서 보다 안전하고 효율적인 운동법이라 판단된다.
Trans Abstract
Although delayed heart rate recovery (HRR) and impaired autonomic nerve system (ANS) modulation after acute exercise are related with cause of cardiovascular disease (CVD) and mortality, studies evaluating ANS changes with local exercise are still unsatisfied. Thus, this study aimed at investigating the modulation of ANS-related parameters, followed by upper or lower body exercise. Eleven male without cardiovascular and orthopedic diseases measured basic body composition, resting blood pressure (BP), and heart rate variability (HRV). This study based on randomized cross-over design; AE composed with arm-ergometer, and LE involved with leg cycling. Participants had at least one week wash-out between each exercise, also there was no cool-down after exercise. All sessions were performed with intensity of 50 % target heart rate for 30 min. With measurement of Rating of perceived exertion (RPE) during every 10 min, HRV was measured Kubios HRV software using R-R intervals collected with Polar RS800CX in post-exercise recovery (for 30 min). As a result, heart rate (HR) and RPE were same (p > 0.05) through the experiment. As results of this study, SDNN and rMSSD in time domain on LE were higher than on AE during post-exercise recovery. When LE compared with AE used by Poincare plot, both parasympathetic reactivation (SD1) and autonomic nerve regulation (SD 2) on LE were higher than AE. Immediately after submaximal exercise, the high-frequency component on LE was significantly greater compared to AE. Also, the LF/HF ratio and LF nu reflecting sympathetic activity were higher on AE than LE. In contrast, the HF/TP ratio and HF nu reflecting vagal tone were greater on LE than AE. In conclusion, this study suggested regional lower body exercise recovers more sufficient than regional upper body exercise after submaximal aerobic exercise at same HR. Local exercise like leg cycling needs a careful approach to apply for accurate exercise prescription and effective training.
서론
외부적 또는 내부적 자극에 의한 심박수의 변이(fluctuation)는 교감신경계(sympathetic nervous system, SNS)와 부교감신경계(parasympathetic nervous system, PNS)로 이루어진 자율신경시스템(autonomic nervous system, ANS)의 지배를 받으며, 이러한 ANS의 활성도 감소 및 SNS의 활동과잉으로 초래된 불균형은 다방면의 질병발생에 관여한다고 알려져 있다(Thayer et al., 2010).
ANS 활동의 평가를 위해 비침습적이며 비용효율적 기법인 심박변이도(heart rate variability, HRV)가 광범위하게 활용되어지고 있으며(Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology, 1996), 실제 대규모 역학 Framingham 심장연구에서 2501명(mean age of 53 years; 1101 men, 1400 women)을 대상으로 평가 분석한 결과 HRV의 감소 및 불균형이 심장사고의 위험증가와 관련하는 것으로 나타났다(Tsuji et al., 1996).
한편 신체적 비활동은 ANS 기능 저하를 유발하는 반면, 정기적인 유산소운동 트레이닝은 심장미주신경모듈을 증가시키고 교감신경활동을 억제하여 심혈관사고 감소에 기여하는 것으로 알려져 있다(Bouchard & Rankinen, 2001). 구체적으로 유산소 운동 시 운동강도를 설정하기 위한 전통적인 접근법으로 최대심박수(maximum heart rate, HRmax) 또는 여유심박수(hear rate reserve, HRR)법 등은 운동자극에 대한 심박수(heart rate, HR) 반응을 이용한다(Mann et al, 2013). 그런데 상지와 하지의 국소적 유산소운동에서 HRmax 또는 HRR법에 따라 HR을 일치시킬 경우 운동양식에 따라 ANS 조절에 차이가 나타난다.
팔은 다리에 비해 상대적으로 active muscle mass의 수준이 낮기 때문에 팔을 이용한 최대운동검사에서 다리 운동에 비해 높은 혈압반응을 보이며 운동 중 최대심박수가 낮게 나타난다(Volianitis & Secher, 2002). 예를 들어 남녀 20명(aged 18 to 45 years; 11 males and 9 females)을 대상으로 최대운동부하검사를 실시한 결과, HRmax가 arm ergometer 수행 시 leg cycling 수행 시에 비해 유의하게 낮은 수준을 나타내었다(Ranadive et al., 2011). 따라서 팔과 다리의 국소적 운동 시 동일한 운동 상태를 설정하기 위하여 HR을 일치시킬 경우, 상대적으로 다리의 운동부하를 가중하게 되는데 이것은 운동 중 ANS 활성도에 영향을 미친다. 예를 들어 파워스펙트럼밀도(power spectral density analysis, PSD) 분석에 의해 산출된 total spectral power[TP]는 ANS의 총 활성도를 반영하는 지수로서 운동자극에서 급격히 감소되는 것으로 알려져 있다(Perini et al., 1990). 실제 활동적인 남자대학생 17명을 대상으로 15분 간의 HR(50% and 60% HRmax)을 일치시킨 평형상태운동(steady state exercise) 동안 산출된 TP는 arm ergometer 에 비해 leg cycling에서 유의하게 감소하였음을 보고하였다(Leicht et al., 2008). 이는 HR을 일치한 다리운동은 상대적으로 높은 운동부하에서 운동을 수행하기 때문에 ANS의 총 활성도가 팔 운동에 비해 감소한다는 것을 시사한다.
이와 대조적으로 14명의 건강한 남성(aged 20 ± 4 years)을 대상으로 에르고미터를 이용하여 점진적 운동부하 테스트를 실시한 결과 동일한 산소소비량(oxygen consumption) 수준에서는 오히려 arm ergometer 운동이 leg cycling 운동에 비해 미주신경활성화를 반영하는 Poincaré plot의 SD1(Mourot et al., 2004)이 급속히 감소된 반면, HR은 유의하게 높은 것으로 나타났다(Tulppo et al., 1999). 따라서 HR을 이용한 유산소 운동처방은 팔과 다리의 국소적 운동에서 운동 시 다른 양상을 보인다.
결국 HR을 일치시킨 다리와 팔의 운동 중 혈역학적 반응 및 ANS 조절을 살펴보면 팔과 다리의 국소적 운동에서 운동강도 설정 시 HR을 이용할 경우 동일한 운동강도에서 활동근육량을 보상하기 위해 팔보다 다리 운동에서 더 높은 부하가 적용된다. 따라서 운동 중 HRV의 감소는 당연히 다리운동에서 더 크게 나타난다(Leicht et al., 2008).
한편 운동자극에 대한 HR 반응 및 ANS 조절은 post-exercise recovery에서 중요한 건강정보를 제공하는데, 실제 post-exercise recovery에서 운동자극으로 유발된 HR의 감소는 ANS 조절에 의존하며, 특히 운동 후 지연된 미주신경재활성화 및 지속적인 SNS 활동은 심장의 이소성 활동(ectopic activity)을 증가시켜 심혈관사고 및 심장돌연사의 위험을 높이는 것으로 알려져 있으며(Albert et al., 2000), 건강한 성인 남녀 2428명(aged 57 ± 12 years; 63% men)의 cohort 연구에서는 최대 운동 후 1분 동안 지연된 HR 감소 및 회복이 모든 사망의 강력한 예측인자임을 보고하였다(Cole et al., 1999). 운동 후 PNS의 재활성화를 포함한 heart rate recovery가 lean muscle mass와 관련한다는 점에서(Buchheit et al., 2011) 비록 HR을 일치시키기 위해 다리의 운동부하가 높았다 하더라도 팔에 비해 활동근육량이 다리가 많기 때문에 실제 국소적 최대하 평형상태운동(submaximal exercise) 후 post-exercise recovery에서 PNS의 재활성화 및 ANS 회복은 실질적 검증이 필요하다. 그러나 HR을 일치시킨 팔과 다리의 최대하(submaximal exercise) 운동 후 post-exercise recovery에서 PNS 재활성화를 포함한 ANS 기능회복의 양상은 알려진 바가 없다.
따라서 본 연구는 HR 수준을 일치시킨 최대하 arm ergometer 및 leg cycling 운동 후 심박회복에 따른 HRV parameter 간의 차이를 비교하는 데 목적이 있으며, 이는 ANS 기능향상의 측면에서 효율적인 운동양식을 탐색하기 위한 기초 정보를 제공하는 데 그 의의가 있다.
연구방법
연구 대상
본 연구는 D 광역시에 소재한 K대학에 재학 중인 남자대학생 11명을 대상으로 수행하였다. 참여자들은 유산소운동 수행에 영향을 미칠 수 있는 근골격계 장애가 없으며, 의료기록상 심혈관질환 및 대사질환이 없는 정상혈압의 건강한 남성로 구성되었다. 본 연구는 경북대학교 윤리위원회의 승인(승인번호: 2014-0066) 하에 수행되었으며 연구원들은 연구의 취지 및 수반되는 위험성을 고지하고 자발적 참여에 관한 동의서에 서명을 받았다. 참여자들의 임상적 특징은 <표 1>과 같다.

Clinical characteristic of participants (n = 11).
실험 방법
모든 피험자는 실험 24시간 전에 알코올 및 카페인 섭취를 제한하고 격렬한 신체활동을 금하도록 지시하였다. 신장 및 체중을 포함한 체조성 및 안정 시 혈압 수준을 측정하고 가벼운 식사 후 적어도 3시간의 휴식을 부여했다. 최대하 운동 전 20분 이상 실험 안정 후 앉은 자세에서 10분 동안 안정 시 R-R intervals를 획득하였다. 무작위 교차설계(randomized cross-over design)에 의해 arm ergometer를 이용한 상체운동(AE)과 leg cycle을 이용한 하체운동(LE)을 각각 수행하였다. AE 또는 LE 수행 후 다음 운동 수행까지 적어도 1주간의 회복기를 부여하였다. post-exercise recovery HRV parameters는 앉은 자세에서 REC 1(after exercise at 0 to 10 min), REC 2(after exercise at 10 to 20 min), REC 3(after exercise at 20 to 30 min)의 세 시기에서 획득하였다.
한편 post-exercise recovery에서 PSD 분석을 통해 frequency power를 산출할 때 반드시 고려해야 할 점이 있다. 안정 시 LF는 교감신경 및 부교감신경의 활동 상태를 동시에 반영하는 반면 HF는 독립적으로 부교감신경활동을 반영하는 것으로 알려져 있다. 그러나 운동자극으로 초래된 HR의 상승은 VO2max 25~30 % 수준에서도 TP를 60% 이상 감소시키며, HF의 경우 안정 시에서 저강도 수준의 운동에서 지속적으로 감소하지만 70% VO2max를 초과하는 운동에서 뚜렷한 변화가 나타나지 않기 때문에 고강도 운동 시 부교감신경저하를 반영할 수 없다. 반면 LF는 중강도 및 고강도 운동에서도 지속적으로 감소하기 때문에 LF/HF ratio는 교감신경활동을 반영한다고 해석할 수 없다(Perini & Veicsteinas, 2003). 따라서 post-exercise recovery의 ANS 활동을 과학적으로 해석하기 위하여 AE 및 LE의 운동 강도를 50% HRR로 heart rate reserve, HRR)로 설정하고, HR이 운동 종료 직후 30 sec~1 min에서 기하급수적으로 감소한다는 점을 고려하여(Imai et al., 1994) REC1에서 운동 직후 0~1 min 동안의 R-R intervals은 HRV parameters의 산출범위에서 제외하였다.
신체조성 측정
참가자들은 속옷을 제외한 의복을 탈의하고 맨발상태로 자동신장·체중계(GL-150, G-TECH International Co., Uijungbu, Korea)를 이용해 신장과 체중을 각각 2회에 걸쳐 측정 후 평균값을 채택하였고, 측정된 신장·체중 값을 이용해 체질량지수(body mass index, BMI)를 산출하였다.
미국스포츠의학회(American College of Sports Medicine, ACSM)의 지침서의 3-point skinfold 프로토콜에 따라 체지방율을 산출하였다. 구체적으로 보정된 아날로그식 skinfold caliper(Dynatronics Co., Salt Lake City, USA)를 이용해 가슴(pectoral), 복부(abdominal), 대퇴(thigh) 부위를 2회 측정 후, 두 값이 2 mm 이상일 경우 재측정 하였으며(ACSM, 2013). 측정된 값을 이용해 Jackson & Pollock의 공식에 따라 체지방률을 산출하였다(Jackson & Pollock, 1978).
Blood Pressure Measurement
12시간 공복 상태로 20분 이상 실험실 안정 후 앉은 자세로 자동혈압측정기(Beurer BM16®, Beurer GmbH, Ulm, Germany)를 이용해 측정시간 간격을 3분으로 mean HR과 함께 systolic blood pressure(SBP) 및 diastolic blood pressure(DBP)를 2회에 걸쳐 측정하였다. 측정 값의 오차가 10 mmHg 이상일 경우 1회 더 측정하여 오차 값이 적은 2개 값 중 낮은 값을 자료로 이용하였다. 채택된 SBP 및 DBP 값을 바탕으로 MAP{mean arterial pressure, MAP = 1/3(SBP) + 2/3(DBP)}를 산출하였다.
최대하 운동 protocol
모든 최대하 운동은 고정식 ergometer(Aerobike 75XLII, Combi Wellness Co. Ltd., Tokyo, Japan)를 이용하여 수행하였으며, AE의 경우 ergometer를 테이블 위에 올려 크랭크 축과 피험자의 어깨 축을 수평으로 일치되도록 설계하였고(Schneider et al., 2002), LE의 경우 무릎의 신전 및 굴곡 시 적합한 페달링을 할 수 있도록 ergometer 안장 높이를 조정하였다.
ACSM의 가이드라인에 따라 카보넨(Karvonen)의 공식을 적용하여 50% HRR 수준으로 목표 심박수(target heart rate, THR)를 설정하여 30분간 운동을 수행하였다(ACSM, 2013).
구체적으로 AE는 15 watts, 60 rev/min의 회전율로, LE는 30 watts, 60 rev/min로 각각 3분간 준비운동 후, 각 70 rev/min의 회전율을 유지한 상태에서 점진적으로 부하를 증가시켜 50% HRR에 도달하도록 유도하였으며(Leicht et al., 2008), 운동 수행동안 무선심박계(Polar RS800cx, Polar Electro, Kemple, Finland)를 이용하여 HR 변화를 지속적으로 모니터링 하였다.
HRV 측정
HRV 분석을 위한 데이터 획득을 위해 온도와 습도를 제어한 조명이 어두운 실험실 환경을 조성하였다(김춘섭과 김맹규, 2014). Interbeat intervals(IBIs)은 안정 시 10분을 포함한 AE 및 LE 세션 종료 후 post-exercise recovery의 REC1, REC2, REC3으로 구성된 세 시기에서 각각 10분간 앉은 자세로 기록되었다. HRV 측정 시 호흡제어에 대한 논쟁이 있으나, 휴식 상태의 HRV 측정 시 호흡 빈도가 영향을 미치지 않는다는 강력한 증거들(Thayer et al 2011)이 제시되어 있기 때문에 본 연구에서는 IBIs 기록 간 참가자들은 자발적인 호흡을 유지하도록 설정했다. IBIs는 1000 Hz로 설정된 Polar RS800CX를 통해, 착용한 chest strap(two-lead)으로부터 무선 기록되었다.
Polar IBIs의 원시 데이터(raw data)는 Pro-trainer Polar 5 software(version 5.40.171, Polar Electro, Kempele, Finland)에 의해 text file(.HRM)로 추출 후 HRV analysis software Kubios(version 2.1, 2012, Biosignal Analysis And Medical Imaging Group, University of Kuopio, Finland, MATLAB)에 이입하였다. 시간 및 주파수 그리고 비선형 지수를 산출하기 전에 artifact correction을 통해 이소성 beat를 배제하고 단기간 HRV 표준검사(5 min) 프로토콜에 따라 256 points/Hz의 연속적인 IBIs를 선별하여 Smoothness priors(Lambda, 500) 기법을 이용한 탈 경향화법(detrended method)을 통해 재추출하였다(Tarvainen et al., 2014).
ANS 기능 및 밸런스를 평가하기 위하여 시간영역의 SDNN(Standard deviation of RR intervals)과 미주신경활동반영지수 rMSSD(Square root of the mean squared differences between successive RR intervals) 및 pNN50(NN50 divided by the total number of RR intervals)을 산출하였다. 또한 PSD 분석을 위해 고속퓨리에 변환(fast Fourier transform)법을 적용하여 저주파(low frequency power, LF, 0.04 - 0.15 Hz)성분 및 고주파성분(high frequency power, HF, 0.15 – 0.4 Hz)을 추출하였다(김철 등, 2006). 한편 비침습적 생체신호는 일반적으로 비정상성(non-stationary)을 내포한 불안정적 성격을 가지기 때문에 최근 비선형기법을 이용한 HRV 해석의 중요성이 대두되고 있으며, 특히 Poincaré plot 분석법은 연속적인 R-R intervals 간의 연관성을 도식화하여 가로축 즉 수평축(transverse axis) 변이를 나타내는 SD1과 세로축 즉 종축(longitudinal axis) 변이를 나타내는 SD2를 통해 ANS를 해석하는 기법으로 단기간 HRV 측정(5 min)에 적용가능하다(Voss et al., 2012). 따라서 본 연구에서는 시간 및 주파수, 추가적으로 Poincaré plot의 parameters를 활용하여 운동양식에 따른 ANS 조절을 비교분석하였다.
운동자각도(ratings of perceived exertion, RPE) 측정
15단계의 Borg scale을 실험 전 충분히 인지하도록 하였으며, 운동 전, 중 및 운동 후, 각각 10분 간격으로 주관적 자각도를 수치화하였다(Borg et al., 1987).
자료 처리 방법
모든 자료 처리는 SPSS Statistics 21.0(Statistical Package for the Social Sciences software, versions 21.0, SPSS Inc., Chicago, Illinois, USA) 프로그램을 사용하여 각 항목별 평균(mean)과 표준오차(standard error)를 산출하였다. 반복측정분산분석(repeated measure ANOVA)을 통해 시간과 운동모드(Arm or Leg) 간의 교호작용을 검증하였으며, 안정 시 및 post-exercise recovery에서 REC1, REC2, REC3의 세 구간 동안 AE와 LE 간의 차이는 대응표본 t-검정(paired t-test)을 이용해 분석하였다. 모든 통계적 유의수준 α = 0.05 미만으로 설정하였다.
결과
안정 시(AE, 67.03 ± 2.95 beats/min; LE, 66.80 ± 3.09 beats/min) 및 Arm ergometer와 Leg cycling 운동 동안 0~10분(AE, 124.45 ± 2.48 beats/min; LE, 124.03 ± 3.40 beats/min), 10~20분(AE, 131.84 ± 1.56 beats/min; LE, 131.24 ± 1.54 beats/min), 20~30분(AE, 133.79 ± 1.58 beats/min; LE, 131.11 ± 1.42 beats/min) 동안의 mean HR에 유의한 차이는 나타나지 않았으며(p>.05), 매 10분 간격으로 측정한 RPE에서도 통계적인 차이(p>.05)는 나타나지 않았다(data not shown).
안정 시 및 post-exercise recovery에서 운동모드에 따른 HRV parameters 간의 차이<표 2>

The difference between arm ergometer and leg cycling on HRV parameters at resting and post-exercise recovery
안정 시 시간 및 주파수 그리고 Poincaré plot indexes에서 통계적인 차이는 나타나지 않았다. 그러나 post-exercise에서 SDNN은 REC1(p<.05) 및 REC2(p<.01) 그리고 REC3(p<.05)에서 각각 유의한 차이가 나타났으며, 반복측정분산분석 결과 운동모드와 시간적 변화에서 유의한 교호작용의 효과가 나타났다(p<.05). 미주신경활성화를 반영하는 rMSSD는 REC1(p<.05)과 REC2(p<.05)의 두 시기에서 각각 LE가 AE에 비해 유의하게 높은 수준을 나타냈다. 또한 REC1에서는 Spectral power parameters에서 독립적으로 PNS 활성화를 반영하는 고주파성분(HF)의 절대 값(absolute value)이 통계적인 차이를 나타냈다(p<.01). 마찬가지로 REC1 및 REC2에서 각각 Poincaré plot의 PNS 활성화지수인 SD1이 AE보다 LE에서 높은 값을 나타냈으며(p<.05), SD2는 post-exercise recovery의 전 구간에서 LE가 AE보다 유의하게 증가하였으며(p<.05), 운동모드와 시간의 변화에서 유의한 교호작용 효과를 나타냈다(p<.05).
운동양식에 따른 안정 시 및 post-exercise recovery에서 Spectral power의 비율(ratio) 변화
ANS 밸런스 해석에 있어서 SNS 우세를 나타내는 저주파 성분과 고주파 성분의 비(LF/HF ratio)는 운동 전 안정 시에서 AE와 LE 간에 통계적인 차이가 없었으나 REC1에서 AE는 LE에 비해 유의하게 높은 수준(p<.05)을 나타냈다. REC2(p>.05)와 REC3(p>.05)에서도 통계적인 차이는 없었으나 AE가 LE에 비해 높은 수준(p>.05)을 나타내었다<그림 1>.
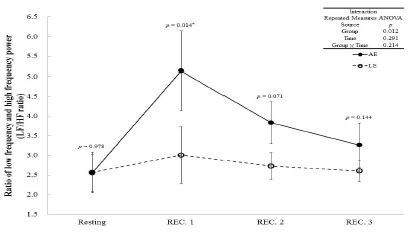
The change of LF/HF ratio in two aerobic exercise modes at resting, and post-exercise recovery (REC) 1, 2, and 3.
Significant difference between arm ergometer(AE) and leg cycling(LE) was deducted from paired t- test. Interaction was obtained by repeated measures analysis of variance (Repeated measures ANOVA).
*p<.05, statistically significant difference between AE and LE
이와 대조적으로 미주신경활동을 동반한 PNS의 재활성화를 보여주는 HF/TP ratio는 안정 시 운동모드 간 유의한 차이가 없었음에도 불구하고 REC1에서 LE가 AE에 비해 HF/TP ratio의 증가가 유의하게 높은 수준을 보여주었다(p<.05). AE와 LE 간의 통계적인 차이는 시간의 경과에 따라 REC2(p>.05) 및 REC3(p>.05)에서는 나타나지 않았다<그림 2>.
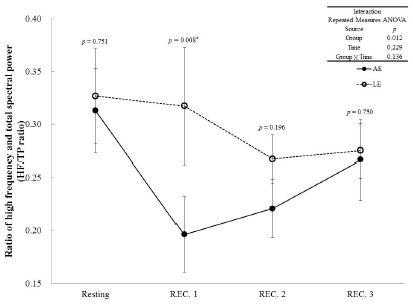
The change of HF/TP ratio in two aerobic exercise modes at resting, and post-exercise recovery (REC) 1, 2, and 3.
Significant difference between arm ergometer(AE) and leg cycling(LE) was deducted from paired t- test. Interaction was obtained by repeated measures analysis of variance (Repeated measures ANOVA).
*p<.05, statistically significant difference between AE and LE
운동양식에 따른 안정 시 및 post-exercise recovery에서 Spectral power의 정규화 수치 변화
ANS 밸런스 해석에 있어서 SNS 우세를 나타내는 저주파 성분의 정규화 값(normalized unit of low frequency power, LF nu)은 안정 시 통계적인 차이가 나타나지 않았으나 REC1에서 AE가 LE에 비해 유의하게 높은 값을 나타내었으며, AE와 LE 간의 통계적인 차이는 시간의 경과에 따라 REC2(p>.05) 및 REC3(p>.05)에서는 나타나지 않았다<그림 3>.
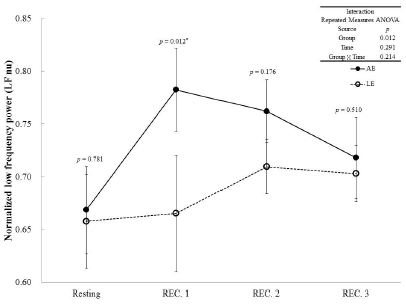
The change of normalized low frequency (LF nu) in two aerobic exercise modes at resting, and post-exercise recovery (REC) 1, 2, and 3.
Significant difference between arm ergometer(AE) and leg cycling(LE) was deducted from paired t- test. Interaction was obtained by repeated measures analysis of variance (Repeated measures ANOVA).
*p<.05, statistically significant difference between AE and LE
post-exercise recovery에서 PNS의 재활성화를 반영하는 고주파 성분의 정규화 값(normalized unit of low frequency power, LF nu)은 안정 시 통계적인 차이가 나타나지 않았으나 REC1에서 LE가 AE에 비해 높은 값을 나타내었으며 AE와 LE 간의 통계적인 차이는 시간의 경과에 따라 REC2(p>.05) 및 REC3(p>.05)에서는 나타나지 않았다<그림 4>.

The change of normalized high frequency (HF nu) in two aerobic exercise modes at resting, and post-exercise recovery (REC) 1, 2, and 3.
Significant difference between arm ergometer(AE) and leg cycling(LE) was deducted from paired t- test. Interaction was obtained by repeated measures analysis of variance (Repeated measures ANOVA).
*p<.05, statistically significant difference between AE and LE
논의
HR을 일치시킨 상·하지의 국소적 운동에서 팔과 다리의 활동근육량 차이로 인해 다리는 팔에 비해 상대적으로 높은 부하에서 운동을 수행하며 이는 ANS활성도에 영향을 미친다. 운동 중 HR은 SNS 활동 촉진 및 PNS 활동 저하로 안정 시에 비해 증가하지만 운동 종료와 함께 SNS활동 감소와 함께 PNS 재활성화로 급격히 감소하는 데 특히 post-exercise recovery에서 나타나는 ANS 회복은 심장사고 및 심혈관질환 등에 대한 중요한 건강정보를 제공한다. 따라서 팔과 다리의 국소적 운동 후 post-exercise recovery에서 나타나는 ANS 조절은 효율적 유산소운동을 위한 중요한 정보를 제공한다.
Carrasco 등에 따르면 전체적인 ANS 활성도를 나타내는 SDNN은 Poincaré plot의 종축 변이(SD2)와 밀접하게 관련하며 미주신경활성화를 반영하는 rMSSD는 수평축 변이(SD1)와 강한 연관성을 가진다(Carrasco et al., 2001). 따라서 post-exercise recovery의 전 시기에서 LE가 AE에 비해 SDNN 및 SD2의 회복수준이 높았다는 것은 하지 운동이 상지 운동에 비해 ANS 활성도 회복이 효율적으로 이루어진다는 것을 시사하며, rMSSD 및 SD1의 수준이 REC1 및 REC2에서 AE에 비해 LE에서 빠르게 회복했다는 것은 하지운동이 상지운동에 비해 운동 후 미주신경의 재활성화가 효율적으로 이루어진다는 사실을 보여준다. 단, rMSSD 및 SD1의 회복 차는 REC3에서 상쇄된다는 점에서 운동양식에 따른 부교감신경재활성화의 차는 운동 후 초기회복단계에서 나타나는 것으로 판단된다.
앞서 언급한 바와 같이 spectral power의 고주파 성분 즉 HF는 동결절(sinus node)에서 PNS 활성도를 반영하며 호흡활동과 직접적으로 관련이 있다(Yamamoto et al., 1995). 반면 저주파 성분 LF는 SNS 활동과 PNS 활동을 동시에 반영하는 혼합지수로 알려져 있으며(Bernardi et al. 1994), 따라서 HF 및 HF와 TP의 비(HF/TP ratio)는 PNS 활동의 반영지수로, LF/HF ratio는 SNS의 활동지수로 이용된다(Yamamoto et al., 1991). post-exercise에서 heart rate recovery와 HRV는 비침습적으로 심장 ANS 조절 특히 PNS 재활성화를 평가하는 보편적인 기법으로 Dupuy 등의 연구에서 30명의 건강한 남성을 대상으로 2회에 걸쳐 6 분간의 최대하 트레드밀 운동 후 10분 간의 post-exercise recovery에서 산출된 HF 및 LF/HF ratio 그리고 HFnu는 높은 내적 신뢰도(intraclass correlation coefficient, ICC; 0.70 < ICC < 0.88)를 나타내었다(Dupuy et al., 2012). 한편 Mendonca 등의 연구에서 유산소운동과 무산소운동을 복합처방한 12주간의 서킷트레이닝 결과 정상인집단과 심혈관질환의 위험이 높은 Down syndrome 환자집단 모두에서 고주파 성분의 정규화 값(HF nu)의 증가와 저주파 성분의 정규화 값(LF nu)이 감소됨으로써 PNS활성 증가 및 SNS 활동의 저하를 통해 운동을 통한 ANS 기능향상을 보고하였다(Mendonca et al, 2013). 본 연구의 결과 초기 post-exercise recovery(REC1)에서 HF 및 HF ratio 그리고 HF nu가 상지운동(AE)에 비해 하지운동(LE)에서 높은 회복을 나타낸 반면, LF/HF ratio 및 LF nu는 하지운동에 비해 상지운동에서 높은 값을 유지했다는 것은 HR을 일치시키기 위해 하지의 국소적 운동이 상지의 국소적 운동에 비해 높은 부하에서 최대하 운동을 수행했음에도 불구하고 운동종료와 함께 구동되는 PNS의 재활성화 및 SNS의 활동저하가 효율적으로 이루어짐을 시사한다. 이러한 회복 차는 시간의 경과에 의해 REC2와 REC3에서 상쇄되지만, Cole 등의 연구에서 알 수 있듯이 운동 종료 직후 지연된 HR의 회복이 심혈관질환을 비롯한 모든 사망률과 관련한다는 관점(Cole et al., 1999)에서 상·하지의 국소 운동에 따른 초기 post-exercise recovery의 회복 차는 임상적으로 중요한 의미를 가진다고 판단된다.
본 연구는 몇몇의 제한점을 가지는 데 첫째 젊은 성인남성만을 대상으로 수행한 결과로서 성 및 연령에 따른 특성을 반영할 수 없다. 실제 HRV를 이용한 ANS 모니터링은 성 및 연령에 의존적이나 특정 동질집단을 통해서 팔과 다리의 국소적 운동 후 ANS의 회복에서 유의미한 결과를 도출했다. 둘째 유산소운동 수행 후 나타나는 ANS 조절을 평가하였기 때문에 저항트레이닝 등 다양한 운동양식을 반영할 수 없다. 그러나 심혈관 및 ANS 기능 향상을 위한 유산소운동의 특성을 규명함으로써 새로운 건강정보를 제공하였다.
결론
건강한 남성 11명을 대상으로 팔과 다리의 국소적 운동 후 ANS의 회복변화를 살펴본 결과 다음과 같은 결과를 도출하였다.
HR 수준을 일치시킨 최대하 arm ergometer 및 leg cycling 실시 후 post-exercise recovery 산출된 HRV parameter 간의 차이를 비교분석한 결과 다음과 같은 결과를 도출하였다.
첫째, 시간영역지수를 이용해 운동양식 간의 차이를 평가한 결과 post-exercise recovery에서 AE 수행 후에 비해 LE 수행 후 ANS 조절능(SDNN) 및 PNS 재활성화(rMSSD)가 높게 나타났다.
둘째, Poincaré plot을 이용해 운동양식 간의 차이를 평가한 결과 post-exercise recovery에서 AE 수행 후에 비해 LE 수행 후 ANS 조절능(SD2) 및 PNS 재활성화(SD1)를 반영하는 HRV parameters의 회복률이 높게 나타났다.
셋째 spectral power에서 PNS 재활성화를 독립적으로 반영하는 HF가 초기 post-exercise recovery(REC1)에서 AE 수행 후에 비해 LE 수행 후 유의하게 증가하였으며, 교감-미주신경 밸런스(sympathetic-vagal balance)에서 SNS 활성화반영지수(LF/HF ratio & LF nu)는 AE 수행 후 유의하게 높은 수치를 나타낸 반면 PNS 활성화반영지수(HF/TP ratio & HF nu)는 LE 수행 후 유의하게 높은 수치를 나타내었다.
이상의 결과에서 젊고 건강한 남성에서 HR을 매치한 팔과 다리의 국소적 운동은 다리에서 상대적으로 높은 부하의 운동을 수행함에도 불구하고 post-exercise recovery에서 다리운동이 팔 운동에 비해 신속하게 ANS 활성도가 회복되며 특히 운동종료 직후에서 미주신경활동을 동반한 PNS의 재활성화가 활발하게 일어남을 알 수 있다. 따라서 ANS 조절 측면에서 하지를 이용한 유산소운동이 상지에 비해 상대적으로 안전하고 효율적인 운동양식이라 판단되며, 추후 성 및 연령 등을 고려한 다양한 인구집단을 통해 추가적인 검증이 필요하다고 생각된다.
References
김철, 방인걸, 김영주(2006). 관상동맥질환에서 안정 시 심박변동 및 최대운동 후 심박수 회복에 대한 베타차단제의 영향. 체육과학연구, 17(3), 23-32.
김 철, 방 인걸, 김 영주. 2006;관상동맥질환에서 안정 시 심박변동 및 최대운동 후 심박수 회복에 대한 베타차단제의 영향. 체육과학연구 17(3):23–32.김춘섭, 김맹규(2014). 단기간의 흡연중단과 유산소운동이 자율신경조절에 미치는 영향. 한국생활환경학회지, 21(3), 364-365.
김 춘섭, 김 맹규. 2014;단기간의 흡연중단과 유산소운동이 자율신경조절에 미치는 영향. 한국생활환경학회지 21(3):364–365.Albert, C. M., Mittleman, M. A., Chae, C. U., Lee, I. M., Hennekens, C. H., & Manson, J. E. (2000). Triggering of sudden death from cardiac causes by vigorous exertion. N Engl J Med, 343(19), 1355-1361.
Albert C. M., Mittleman M. A., Chae C. U., Lee I. M., Hennekens C. H., et al, Manson J. E.. 2000;Triggering of sudden death from cardiac causes by vigorous exertion. N Engl J Med 343(19):1355–1361. 10.1056/nejm200011093431902.American College of Sports Medicine. (2013). ACSM’s guidelines for exercise testing and prescription(9th ed.). Lippincott Williams and Williams, Philadelphia, PA
. American College of Sports Medicine. 2013. ACSM’s guidelines for exercise testing and prescription (9th ed.)th ed. Lippincott Williams and Williams. Philadelphia, PA:Bernardi, L., Leuzzi, S., Radaelli, A., Passino, C., Johnston, J. A., & Sleight, P. (1994). Low-frequency spontaneous fluctuations of R-R interval and blood pressure in conscious humans: a baroreceptor or central phenomenon?Clin Sci (Lond), 87(6), 649-654.
Bernardi L., Leuzzi S., Radaelli A., Passino C., Johnston J. A., et al, Sleight P.. 1994;Low-frequency spontaneous fluctuations of R-R interval and blood pressure in conscious humans: a baroreceptor or central phenomenon? Clin Sci (Lond) 87(6):649–654.Borg, G., Hassmén, P., & Lagerström, M. (1987). Perceived exertion related to heart rate and blood lactate during arm and leg exercise.Eur J Appl Physiol Occup Physiol, 56(6), 679-685.
Borg G., Hassmén P., et al, Lagerström M.. 1987;Perceived exertion related to heart rate and blood lactate during arm and leg exercise. Eur J Appl Physiol Occup Physiol 56(6):679–685. 10.1007/bf00424810.Bouchard, C., & Rankinen, T. (2001). Individual differences in response to regular physical activity.Med Sci Sports Exerc, 33(6), S446-451; discussion S452-453.
Bouchard C., et al, Rankinen T.. 2001;Individual differences in response to regular physical activity. Med Sci Sports Exerc 33(6):S446–451. discussion S452-453. 10.1097/00005768-200106001-00013.Buchheit, M., Al, Haddad. H., Mendez-Villanueva, A., Quod, M. J., & Bourdon, P. C. (2011). Effect of maturation on hemodynamic and autonomic control recovery following maximal running exercise in highly trained young soccer players.Front Physiol, 2(69), eCollection.
Buchheit M., Al Haddad. H., Mendez-Villanueva A., Quod M. J., et al, Bourdon P. C.. 2011;Effect of maturation on hemodynamic and autonomic control recovery following maximal running exercise in highly trained young soccer players. Front Physiol 2(69)eCollection. 10.3389/fphys.2011.00069.Carrasco, S., Gaitan, M. J., Gonzalez, R., & Yanez, O. J. (2001). Correlation among Poincare plot indexes and time and frequency domain measures of heart rate variability.Med Eng Technol, 25(6), 240-248.
Carrasco S., Gaitan M. J., Gonzalez R., et al, Yanez O. J.. 2001;Correlation among Poincare plot indexes and time and frequency domain measures of heart rate variability. Med Eng Technol 25(6):240–248.Cole, C. R., Blackstone, E. H., Pashkow, F. J., Snader, C. E., & Lauer, M. S. (1999). Heart-rate recovery immediately after exercise as a predictor of mortality.N Engl J Med, 341(18), 1351-1357.
Cole C. R., Blackstone E. H., Pashkow F. J., Snader C. E., et al, Lauer M. S.. 1999;Heart-rate recovery immediately after exercise as a predictor of mortality. N Engl J Med 341(18):1351–1357. 10.1056/nejm199910283411804.Dupuy, O., Mekary, S., Berryman, N., Bherer, L., Audiffren, M., & Bosquet, L. (2012). Reliability of heart rate measures used to assess post-exercise parasympathetic reactivation.Clin Physiol Funct Imaging, 32(4), 296-304.
Dupuy O., Mekary S., Berryman N., Bherer L., Audiffren M., et al, Bosquet L.. 2012;Reliability of heart rate measures used to assess post-exercise parasympathetic reactivation. Clin Physiol Funct Imaging 32(4):296–304. 10.1111/j.1475-097x.2012.01125.x.Imai, K., Sato, H., Hori, M., Kusuoka, H., Ozaki, H., Yokoyama, H., Takeda, H., Inoue, M., & Kamada, T. (1994). Vagally mediated heart rate recovery after exercise is accelerated in athletes but blunted in patients with chronic heart failure.J Am Coll Cardiol, 24(6), 1529-1535.
Imai K., Sato H., Hori M., Kusuoka H., Ozaki H., Yokoyama H., Takeda H., Inoue M., et al, Kamada T.. 1994;Vagally mediated heart rate recovery after exercise is accelerated in athletes but blunted in patients with chronic heart failure. J Am Coll Cardiol 24(6):1529–1535. 10.1016/0735-1097(94)90150-3.Jackson, A. S., & Pollock, M. L. (1978). Generalized equations for predicting body density of men.Br J Nutr, 40(3), 497-504.
Jackson A. S., et al, Pollock M. L.. 1978;Generalized equations for predicting body density of men. Br J Nutr 40(3):497–504. 10.1079/bjn19780152.Leicht, A. S., Sinclair, W. H., & Spinks, W. L. (2008). Effect of exercise mode on heart rate variability during steady state exercise.Eur J Appl Physiol, 102(2), 195-204.
Leicht A. S., Sinclair W. H., et al, Spinks W. L.. 2008;Effect of exercise mode on heart rate variability during steady state exercise. Eur J Appl Physiol 102(2):195–204. 10.1007/s00421-007-0574-9.Mann, T., Lamberts, R. P., & Lambert, M. I. (2013). Methods of prescribing relative exercise intensity: physiological and practical considerations.Sports Med, 43(7), 613-625.
Mann T., Lamberts R. P., et al, Lambert M. I.. 2013;Methods of prescribing relative exercise intensity: physiological and practical considerations. Sports Med 43(7):613–625. 10.1007/s40279-013-0045-x.Mendonca, G. V., Pereira, F. D., & Fernhall, B. (2013). Heart rate recovery and variability following combined aerobic and resistance exercise training in adults with and without Down syndrome.Res Dev Disabil, 34(1), 353-361.
Mendonca G. V., Pereira F. D., et al, Fernhall B.. 2013;Heart rate recovery and variability following combined aerobic and resistance exercise training in adults with and without Down syndrome. Res Dev Disabil 34(1):353–361. 10.1016/j.ridd.2012.08.023.Mourot, L., Bouhaddi, M., Perrey, S., Rouillon, J. D., & Regnard, J. (2004). Quantitative Poincaré plot analysis of heart rate variability: effect of endurance training.Eur J Appl Physiol, 91(1), 79-87.
Mourot L., Bouhaddi M., Perrey S., Rouillon J. D., et al, Regnard J.. 2004;Quantitative Poincaré plot analysis of heart rate variability: effect of endurance training. Eur J Appl Physiol 91(1):79–87. 10.1007/s00421-003-0917-0.Perini, R., & Veicsteinas, A. (2003). Heart rate variability and autonomic activity at rest and during exercise in various physiological conditions.Eur J Appl Physiol, 90(3-4):317-25.
Perini R., et al, Veicsteinas A.. 2003;Heart rate variability and autonomic activity at rest and during exercise in various physiological conditions. Eur J Appl Physiol 90(3-4):317–25. 10.1007/s00421-003-0953-9.Perini, R., Orizio, C., Baselli, G., Cerutti, S., Veicsteinas, A. (1990). The influence of exercise intensity on the power spectrum of heart rate variability.Eur J Appl Physiol Occup Physiol, 61(1-2), 143-148.
Perini R., Orizio C., Baselli G., Cerutti S., Veicsteinas A.. 1990;The influence of exercise intensity on the power spectrum of heart rate variability. Eur J Appl Physiol Occup Physiol 61(1-2):143–148. 10.1007/bf00236709.Ranadive, S. M., Fahs, C. A., Yan, H., Rossow, L. M., Agiovlasitis, S., & Fernhall, B. (2011). Heart rate recovery following maximal arm and leg-ergometry.Clin Auton Res, 21(2), 117-120.
Ranadive S. M., Fahs C. A., Yan H., Rossow L. M., Agiovlasitis S., et al, Fernhall B.. 2011;Heart rate recovery following maximal arm and leg-ergometry. Clin Auton Res 21(2):117–120. 10.1007/s10286-010-0094-2.Schneider, D. A., Wing, A. N., & Morris, NR. (2002). Oxygen uptake and heart rate kinetics during heavy exercise: a comparison between arm cranking and leg cycling.Eur J Appl Physiol, 88(1-2), 100-106.
Schneider D. A., Wing A. N., et al, Morris NR.. 2002;Oxygen uptake and heart rate kinetics during heavy exercise: a comparison between arm cranking and leg cycling. Eur J Appl Physiol 88(1-2):100–106. 10.1007/s00421-002-0690-5.Tarvainen, M. P., Niskanen, J. P, Lipponen, J. A., Ranta-Aho, P. O., & Karjalainen, P. A. (2014). Kubios HRV--heart rate variability analysis software.Comput Methods Programs Biomed, 113(1), 210-220.
Tarvainen M. P., Niskanen J. P, Lipponen J. A., Ranta-Aho P. O., et al, Karjalainen P. A.. 2014;Kubios HRV--heart rate variability analysis software. Comput Methods Programs Biomed 113(1):210–220. 10.1016/j.cmpb.2013.07.024.Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. (1996). Heart rate variability: standards of measurement, physiological interpretation and clinical use.Circulation, 93(5), 1043-1065.
Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology.. 1996;Heart rate variability: standards of measurement, physiological interpretation and clinical use. Circulation 93(5):1043–1065.Thayer, J. F., Loerbroks, A., & Sternberg, E. M. (2011). Inflammation and cardiorespiratory control: the role of the vagus nerve.Respir Physiol Neurobiol, 178(3), 387-394.
Thayer J. F., Loerbroks A., et al, Sternberg E. M.. 2011;Inflammation and cardiorespiratory control: the role of the vagus nerve. Respir Physiol Neurobiol 178(3):387–394. 10.1016/j.resp.2011.05.016.Thayer, J. F., Yamamoto, S. S., & Brosschot, J. F. (2010). The relationship of autonomic imbalance, heart rate variability and cardiovascular disease risk factors.Int J Cardiol, 141(2), 122-131.
Thayer J. F., Yamamoto S. S., et al, Brosschot J. F.. 2010;The relationship of autonomic imbalance, heart rate variability and cardiovascular disease risk factors. Int J Cardiol 141(2):122–131. 10.1016/j.ijcard.2009.09.543.Tsuji, H., Larson, M. G., Venditti, F. J. Jr., Manders, E. S., Evans, J. C., Feldman, C. L., & Levy, D. (1996). Impact of reduced heart rate variability on risk for cardiac events.The Framingham Heart Study. Circulation, 94(11), 2850-2855.
Tsuji H., Larson M. G., Venditti F. J. Jr., Manders E. S., Evans J. C., Feldman C. L., et al, Levy D.. 1996;Impact of reduced heart rate variability on risk for cardiac events. The Framingham Heart Study. Circulation 94(11):2850–2855. 10.1161/01.cir.94.11.2850.Tulppo, M. P., Mäkikallio, T. H., Laukkanen, R. T., & Huikuri, H. V. (1999). Differences in autonomic modulation of heart rate during arm and leg exercise.Clin Physiol, 19(4), 294-299.
Tulppo M. P., Mäkikallio T. H., Laukkanen R. T., et al, Huikuri H. V.. 1999;Differences in autonomic modulation of heart rate during arm and leg exercise. Clin Physiol 19(4):294–299. 10.1046/j.1365-2281.1999.00180.x.Volianitis, S., & Secher, N. H. (2002). Arm blood flow and metabolism during arm and combined arm and leg exercise in humans.J Physiol, 544(Pt 3), 977-984.
Volianitis S., et al, Secher N. H.. 2002;Arm blood flow and metabolism during arm and combined arm and leg exercise in humans. J Physiol 544(Pt 3):977–984. 10.1113/jphysiol.2002.023556.Voss, A., Heitmann, A., Schroeder, R., Peters, A., & Perz, S. (2012). Short-term heart rate variability--age dependence in healthy subjects.Physiol Meas, 33(8):1289-1311.
Voss A., Heitmann A., Schroeder R., Peters A., et al, Perz S.. 2012;Short-term heart rate variability--age dependence in healthy subjects. Physiol Meas 33(8):1289–1311. 10.1088/0967-3334/33/8/1289.Yamamoto, Y., Hughson, R. L., & Peterson, J. C. (1991). Autonomic control of heart rate during exercise studied by heart rate variability spectral analysis.J Appl Physiol, 71(3), 1136-1142.
Yamamoto Y., Hughson R. L., et al, Peterson J. C.. 1991;Autonomic control of heart rate during exercise studied by heart rate variability spectral analysis. J Appl Physiol 71(3):1136–1142. 10.1152/jappl.1991.71.3.1136.Yamamoto, Y., Nakamura, Y., Sato, H., Yamamoto, M., Kato, K., & Hughson, R. L. (1995). On the fractal nature of heart rate variability in humans: effects of vagal blockade.Am J Physiol, 269(4 Pt 2), R830-837.
Yamamoto Y., Nakamura Y., Sato H., Yamamoto M., Kato K., et al, Hughson R. L.. 1995;On the fractal nature of heart rate variability in humans: effects of vagal blockade. Am J Physiol 269(4 Pt 2):R830–837. 10.1152/ajpregu.1995.269.4.r830.