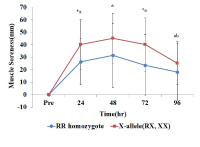
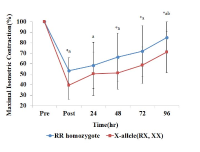
[Purpose] The purpose of this study was to examine the change of muscle damage markers after maximal eccentric exercise and to verify the difference of recovery according to ACTN3 gene polymorphism. [Methods] Fifty healthy males participated in this study. Subjects performed 25 times/1 set (total 2 set) maximal eccentric contractions of the elbow flexor muscles on a modified preacher curl machine with a between-sets rest time of 5 min. Maximal isometric contraction (MIC) was measured 6 times (pre, post, after 24 h, 48 h, 72 h and 96 h). Muscle soreness (SOR) was measured 5 times (pre, after 24 h, 48 h, 72 h and 96 h). Blood samples were collected 5 times (pre, after 24 h, 48 h, 72 h and 96 h). ACTN3 gene polymorphisms were identified using polymerase chain reaction (PCR). Data were analyzed using a 2-way repeated measure ANOVA and post hoc Bonferroni test. [Results] Analysis of ACTN3 gene polymorphism revealed the following distribution: 22% RR (n=11), 50% RX (n=25), and 28% XX (n=14). Individuals were classified into the RR homozygote group (n=11) and the X-allele group (n=39). MIC showed a significant difference between groups and interaction (p<.05). The groups differed significantly in MIC at 48 h, 72 h, and 96 h after exercise and the X-allele group decreased more than the RR homozygote group. The groups differed significantly in muscle soreness and interaction (p<.05). SOR in the X-allele group was significantly higher than in the RR homozygote group at 24 h after exercise. Although blood CK activity was lower in the RR homozygote group than in the X-allele group, but there was no significant difference between the groups (p>.05). [Conclusion] The RR homozygote group showed lower muscle strength reduction rate, muscle soreness and blood CK activity than the X-allele group. This indicates that RR individuals have a lower risk of exercise-induced muscle damage than those with an X-allele.


Purpose The purpose of this study was to investigate the effect of vibration therapy on the functional, imaging, and mechanical properties in elbow flexor after a single bout eccentric exercise. Methods Twenty-three untrained adults male participated in this study [CON(control)= 11, VT(vibration)= 12]. Volunteers performed 5-set of 6 maximal (90˚/s) eccentric contractions of the non-dominant elbow flexor on a isokinetic dynamometer. Vibration was applied using a side alternating vibratory platform (12 Hz frequency, 4 mm amplitude) with 3-set of 60 sec during 3-day after eccentric exercise. Results The VT group showed a reduction in exercised-induced muscle damage(EIMD) symptoms in the form of attenuating muscle swelling and echo intensity (P<.05) compared with the CON, mechanical properties were improvement (P<.05) compared with the CON. However, muscle soreness, range of motion and maximal voluntary isometric contraction were not significant (P<.05). Conclusion As currently practiced, vibration therapy after eccentric exercise may reduce EIMD by improving quality of the muscle, suggesting that this therapy is an effective strategy for EIMD.




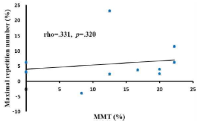
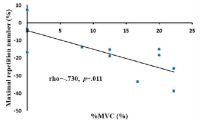
The purpose of this study was to determine whether maximum repetition number can be used as an indicator of strength imbalance. Eleven healthy, resistance-trained males were tested for one repetition maximum (1-RM) the chest-press exercise, and than manual muscle testing (MMT), two-arm at 80% of 1-RM and one-arm at 40% of 1-RM in the pectoralis major were measured for the maximum voluntary contraction (%MVC) and maximum number of repetitions during the chest press exercise. Exercise velocity was constantly 4 seconds (concentric: 2-s, eccentric: 2-s) per repetition. The changes in %MVC were significantly higher in non-dominant limb (NDL) compared with dominant limb (DL) pectoralis major during two-arm chest press (p < 0.01) and one-arm chest press exercise (p < 0.05). In contrast, the changes in MMT (p < 0.05) and maximum repetition number (p < 0.01) were significantly higher in DL compared with NDL during one-arm chest press exercise. There was no correlation between maximum repetition number and MMT (rho = 0.331, p = 0.320). However, maximum repetition number was significantly negative correlated with %MVC in two-arm chest press (rho = -0.730, p = 0.011). It is possible that maximum repetition number can be used as an indicator of strength imbalance.