
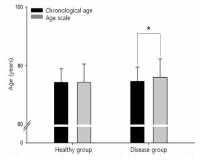
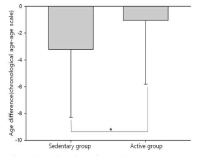
Purpose Evaluating the aging of senior and providing optimal sevices are important things for successful aging. This study identified functional fitness related with heath of aged 65 years or older and developed an age scale (longevity fitness age) for assessing their aging. Methods Participants were 458 older people (166 male, 292 female). They were divided into healthy group and disease group. Healthy group was used for the development of the longevity age equation and disease group was for investigating the validity of the equation. Participants completed 13 function fitness variables. The first principal component obtained from a principal component analysis was used to compute the equation. All variables except for grip strength and carrying beans were correlated with chronological aged. Grip strength and variables related lower functional fitness had differences between healthy group and disease group. Finally, 4 variables were selected for the equation. Results It was the following: longevity fitness age=0.942*X1+2, 185*X2+0.673*X3+0.051*X4+0.588*chronological age+58.401, where X1=standing up from a supine position, sec (s), X2=maximum walking (s), X3=standing up and sitting down a chair (s), X4=one leg balance with eyes open (s). The longevity fitness age of healthy group do not have a difference compared to their chronological age but disease group had a difference significantly. Age difference (chronological age-longevity fitness age) of sedentary group in disease group was significantly bigger than its active group. Longevity fitness age could assess an aging of senior. Conclusion We suggest that it can use as the tool for early detecting senior who need the health care service.

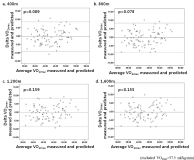
Purpose The purpose of this study was to develop the new indirect method assessing maximal oxygen uptake (VO2max) using heart rate (HR) and accelerometer during walk exercise. Methods One hundred seven participants (55 male, 52 female) performed a graded exercise test to determine VO2max and two types of 1,600 m walk exercises (fast walk and pace controlled walk). The equations for estimating VO2max was developed by stepwise multiple regression. The validity of developed equations tested through the correlation between measured VO2max and estimated VO2max, was assessed by predicted residual sum of squares, and Bland-Altman plotting. Results VO2maxwas correlated with time, and HR/activity count per minute (ACM) measured in pace controlled walk exercise at all distance (400 m, 800 m, 1,200 m, 1,600 m). The equations were valid significantly and their multiple correlation coefficients or standard estimated error were similar to that Åstrand-Rhyming cycle ergometer test or Rockport 1 mile walk test. Using HR/ACM in pace controlled walk (400 m), it was possible to estimate VO2max(R2: 0.675, %SEE: 10.7). The equation was: VO2max=121.659+6.656×Gender-0.865×Age-9.540×Time-2460.952×HR/ACM (Gender, 0=female, 1=male: Time, hundredth of a minute: HR, heart rate: ACM, activity count per minute). Conclusion Estimation equations developed in this study are considered to estimate VO2max through a shorter distance, or a lower intensity of walk exercise. It is required studies to target a wide range of ages or to develop walk test on a lower bpm.

The purpose of this study was a investigate the endothelial function of prehypertensive during dynamic exercise. Hypothesis of this study was to impair the endothelial function in prehypertensive compared to normtensive during dynamic handgrip exercise. Eleven healthy prehypertension (24±2 yrs) and ten healthy normotensive (25 ± 2 yrs) were recruited in this study. Participants were performed dynamic handgrip exercise in one contraction per second at 30% of maximum voluntary contraction for three minutes. Vascular (blood vessel diameter, blood flow) and cardiar response (stroke volume, heart rate and cardiac output) were measured at rest and during exercise. Flow mediated dilation (FMD) was decrease significantly in prehypertensive less than normotensive (p<0.05) at rest, and vasodilation of prehypertensive was reduced significantly less than normitensive during exercise (p<0.05). All the cardiovascular responses were aot significantly different at rest and during exercise between prehypertensive and normotensive. These results suggest that endothelial function is impaired in prehypertensive compared to in normotensive