PURPOSE This study aimed to investigate the effects of accelerated rehabilitation exercise on physical fitness, lower extremity isometric strength, and blood variables in older adult women diagnosed with degenerative osteoarthritis. METHODS A total of 29 older adult women diagnosed with degenerative osteoarthritis residing in G city participated in the study, and 19 participants, excluding dropouts, took part in the experiment. They underwent exercise twice a week for 60 minutes per session over a period of 12 weeks. Pre- and post-experiment, the older adult fitness assessment (SFT), lower extremity isometric strength, and blood variables were measured. Data analysis was performed using SPSS 25.0, and paired sample t-tests were conducted to examine the effects before and after exercise. RESULTS The study results showed significant differences in body mass index (BMI) before and after exercise (p<0.05), and the older adult fitness assessment (SFT) showed significant differences in all items (p<0.01). Lower extremity isometric strength showed significant differences in absolute (Nm) and relative (%BW) values of 20° right flexion muscle (p<0.01). In terms of blood variables, significant differences were observed in creatine and ESR before and after exercise (p<0.01). CONCLUSIONS This study’s results suggest that regular physical activity and rehabilitation exercise programs can positively impact the muscular strength, cardiovascular endurance, exercise function, and blood composition of older adult women diagnosed with degenerative osteoarthritis. It is indicated that conducting future research, including periodic exercise programs, could be beneficial in promoting sustained exercise participation.
The frailty, characterized by reduced physiological function is closely related to a fall, disability, institutionalization, hospitalization, and mortality in the elderly. A reduced physical fitness is a major phenotype of the frailty. The purpose of this study was to investigate the relationship among pre-frailty, physical activity (PA) and functional fitness in the community dwelling elderly women. The study participants were elderly women (n=338, 70.6±4.2years) aged over 65 who took part in the Korean Healthy Fitness Criteria study for the National Fitness Award Project in 2015. The pre-frailty was defined using the Cardiovascular Health Study frailty criteria. PA was assessed using the International PA Questionnaire (IPAQ). The participants were classified as regular PA participants if they meet the World Health Organization (WHO) PA recommendation for the elderly. Functional fitness was assessed using the composite of the National Fitness Award fitness testing for the elderly. Quality of life was evaluated using EuroQoL visual analogue scale and WHO quality of life assessment. As the results, the pre-frail elderly women were significantly older and obese (body mass index, percent body fat, waist circumference) than the healthy elderly. The pre-frail elderly presented significant decreases in walking, moderate intensity, and total PA compared to the healthy elderly even after adjusted for age and percent body fat. However, no significant difference was found in vigorous-intensity activity between the pre-frail and healthy elderly. Also, the pre-frail elderly women showed the decrease in functional fitness and quality of life compared to the healthy elderly. Regular PA was associated with high levels of muscular endurance and coordination in healthy and pre-frail elderly. In pre-frail elderly, high levels of cardiorespiratory endurance was associated with PA. In conclusion, regular PA is inversely associated with fitness decline in healthy and pre-frail community-dwelling elderly women. Regular PA might attenuate fitness decline in pre-frail elderly women.

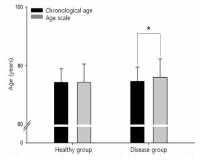
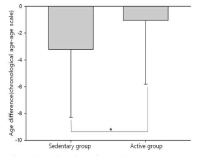
Purpose Evaluating the aging of senior and providing optimal sevices are important things for successful aging. This study identified functional fitness related with heath of aged 65 years or older and developed an age scale (longevity fitness age) for assessing their aging. Methods Participants were 458 older people (166 male, 292 female). They were divided into healthy group and disease group. Healthy group was used for the development of the longevity age equation and disease group was for investigating the validity of the equation. Participants completed 13 function fitness variables. The first principal component obtained from a principal component analysis was used to compute the equation. All variables except for grip strength and carrying beans were correlated with chronological aged. Grip strength and variables related lower functional fitness had differences between healthy group and disease group. Finally, 4 variables were selected for the equation. Results It was the following: longevity fitness age=0.942*X1+2, 185*X2+0.673*X3+0.051*X4+0.588*chronological age+58.401, where X1=standing up from a supine position, sec (s), X2=maximum walking (s), X3=standing up and sitting down a chair (s), X4=one leg balance with eyes open (s). The longevity fitness age of healthy group do not have a difference compared to their chronological age but disease group had a difference significantly. Age difference (chronological age-longevity fitness age) of sedentary group in disease group was significantly bigger than its active group. Longevity fitness age could assess an aging of senior. Conclusion We suggest that it can use as the tool for early detecting senior who need the health care service.
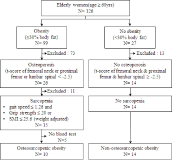
Purpose The purpose of this study were to assess physiological and biochemical characteristics in elderly women with osteosarcopenic obesity (OSO), and to analyze relationships among irisin, adipokines and bone metabolism markers. Methods 126 elderly women were selected and among them 10 women were classified into OSO group (76.9±5.2 yrs) and 14 women were classified as a NOSO group (72.9±5.6 yrs). Physique, body composition and bone mineral density were measured. Senior fitness tests were 30-s chair stand, 30-s arm curl, chair sit-and-reach, back scratch, 8-foot up-and-go, grip strength, and 2-min step test. Isokinetic muscle strength was measured by isokinetic dynamometer (Cybex 770, USA). Nutrition intake and physical activity were administered. Biochemical parameters including irisin, FNDC-5, leptin, adiponectin, CTx, 25(OH)D, osteocalcin, and PTH were measured. All data were analyzed by SAS 9.4. Independent t-test was applied to compare between OSO and NOSO groups. Multiple regression analysis was used. The level of significance was set at .05. Results The results of the study showed that there were significantly high for waist circumference, hip circumference, WHR, and BMI in OSO group compared to those of NOSO group. Higher results were also obtained for fat tissue and percent body fat but significantly low for lumbar bone mineral density. OSO group showed significant lower results for grip strength and 2-min step test compared to NOSO group. Peak torque, and relative peak torque at 60° were significantly lower for left and right knee flexion in OSO group. Protein intake was significantly low in OSO group, but no difference was obtained in level of physical activity between two groups. Irisin was significantly related to adiponectin, FNDC-5 and osteocalcin in explaining 35.2%, 81.5% and 92.1% of the variance, respectively. Conclusions This study shows that elderly women with OSO have higher results for physique and body composition parameters except body height. However, lower values were obtained for functional fitness, and isokinetic muscle strength. OSO may have more risks for metabolic syndrome, bone fractures, fall, lack of daily physical activity and limit of locomotion due to the imbalance of quadriceps and biceps femoris in non dominant leg. This study suggests that criteria and mechanism of OSO should be clarified by follow-up study.